This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This
article is available from https://jpalliativecare.com/2017-iapcon-abstracts/Day 1: Plenary 1: Quality Measurement and Audits - Does Implementing Standards Add Value in Palliative Care Practice?LorenzKarl123Stanford Palliative Care Programs, California, USADepartment of Medicine, Stanford School of Medicine, California, USA E-mail: kalorenz@stanford.eduVA Palliative Care Quality Improvement Resource Center, VA Palo Alto, California, USA
Measurement: Making the Invisible Visible: The practice of palliative care as well as the goals of measurement are founded in the recognition of universal human dignity. Although every human being is endowed with dignity, illness progressively robs us of our agency and often renders us silent and increasingly hidden from view. Furthermore, the challenges we experience such as symptoms and struggles to obtain clear information about our future are imperceptible, as healthcare records rarely document these issues in clear ways and, in fact, many issues that are critical to quality of life are hard to represent (e.g., loneliness or isolation). Measurement is therefore crucial, to make both seriously ill persons and the challenges they face more apparent and actionable. Measurement is a crucial part of improving palliative care, but it is only one aspect of complex interventions that are typical of major efforts to change practice. There have been many rigorous randomized controlled studies of audits alone, and reviews of this evidence suggest that audits are effective although they typically have modest effect sizes and vary considerably in effectiveness. A recent effort synthesized information from many rigorous studies that have been conducted as well as practitioners and researchers and identified many helpful distinctions in crafting effective audits. These lessons have been summarized in 15 important features that address the recipient, format, specificity, actionability, and context among other features for delivering feedback. The United States Department of Veterans Affairs illustrates how these features have worked together to bring coherence and improve performance over time. As India considers national standards, it has a chance to both build on the lessons of other national health systems, but also to innovate beyond them to develop approaches to measurement and accountability that account for important features of the Indian context (e.g., community resources and supports), and facilitate innovation around models of palliative care (e.g., lay health workers).
Keywords: Audit; community care; measurement; Quality improvement
Day 1: Plenary 2: Palliative Care is Everybody's Business. What Can India Learn from the Gold Standards Framework Experience in the UK?ThomasKeri1The Gold Standards Framework Centre, End of Life Care, University of Birmingham, Birmingham, United Kingdom E-mail: keri.thomas@gsfcentre.co.uk
In the context of the international demographic changes, most countries face the challenge of resetting their healthcare systems to care for an ageing population living longer with increased co-morbidities- we live longer but with extended ill health. Nations have focussed on improving early life care for babies and children, provided care for the middle-aged or fit elderly with acute reversible conditions, but struggle with the required reframing of care for people with life-limiting conditions where survival is not the key goal. With demographic challenges now reaching tipping point, we now need to radically re- focus on care for people in the last chapter or final years of their lives, on living well before we die, known in the UK as ‘end of life care’. This growing group of people have a considerable impact on health and social care provision and consume a disproportionate amount of resources, some of which is unwanted and inappropriate, reflecting a trend for potential over-medicalisation and over-hospitalisation in many nations. Meeting this challenge and caring for people nearing the end of their lives, helping them to live well until they die, requires a rethink of our concepts of elderly care, specialist/generalist palliative, hospice and end of life care and a mobilising of our workforce to release talents of all – this is everybody's business. Palliative care demonstrates what can be achieved for some people. But what do we all need to do to be fit for purpose for 21st century demands and meet the challenge of the ageing population? With reducing healthcare funding, our workforce is our strength and could provide the answer- but we need to do things differently and, working with other care providers, systematically reframe and mobilise all generalist frontline teams in every setting.
The Gold Standards Framework (GSF) quality improvement programmes have been extensively used in the UK for the past 20 years to improve care for people with any condition, in any setting, given by any generalist frontline care provider- aspiring to a ‘gold standard’ of care for all. GSF take a population-based approach to end of life care, focusing on the 1% of the population in their last year of life, encouraging pro-active, person-centred systematic care – with practical means to give the right person the right care at the right time in the right place, every-time. We develop organisational learning, tools, resources, measures and support to help identify patients early, assess their needs and preferences and plan provision of tailored care in alignment with their needs and preferences, in a cost effective and efficient way, given by every health and social care provider. With India's changing demography, economic prosperity and growing strength in palliative care, can we extend these concepts to meet the changing needs of the population and, building on lessons learnt in the UK, ensure gold standard care for all?
Keywords: Ageing; end of life care; quality improvement
Day 2: Plenary 3: End of Life Care: The International Collaborative for Best Care of the Dying PersonMacadenStanleyWilkinsonSusieEllershawJohnBangalore Baptist Hospital, Bengaluru, Karnataka, India E-mail: stancmac@gmail.com
Introduction: Death is inevitable but the manner in which a person dies is fundamental to the person concerned and their nearest and dearest. The effects of poor care leading to death are distressing for patients and also have long term effects for those closest to the patient. Sadly, end of life care remains under resourced and funded not only in terms of service provision but equally in research funding.
This paper describes the work of a group of committed International health care professionals whose mission is to improve the care for the dying by sharing their knowledge expertise and engaging in Collaborative innovation research and education. The group, known as The International Collaborative for Best Care for the Dying Person was officially formed in January 2014. The Coordinating Centre for the Collaborative is based at the Marie Curie Palliative Care Institute Liverpool (MCPCIL), University of Liverpool, UK.
Collaborative Vision: The vision of the Collaborative is for a world where all people experience a good death as an integral part of their individual life, supported by the very best personalised care.
Background of the Collaborative: An international meeting was held in Liverpool, UK, November 2013, attended by leading thinkers, practitioners, and researchers in care for the dying from 12 countries. The group had been working together for a number of years with a shared focus on the Liverpool Care Pathway for the Dying Patient (LCP) International Continuous Quality Improvement Programme[1] to drive up the quality for care for the dying in the last few days and hours of life at the clinical interface.
In 2009 the LCP became the focus of the societal debate across print and broadcast media in England. Despite a randomized control trial (RCT) in Italy which, although underpowered, found an overall improvement for patients who were cared for in wards where the LCP was used (Costantini et al., 2014),[2] and the finding of the Neuberger Review into the LCP,[3] which highlighted the ethical basis of the LCP and its efficacy when used appropriately, the LCP was withdrawn from use in England with effect from July 2014.
The international group had also been working together on a wider suite of work packages related to research and development and knowledge transfer related to care for the dying person. The group was successful in securing funding by an EU FP7 Co-ordination and Support Action grant of €2.2million to optimise research for the care of cancer patients in the last days of life. This collaborating project was called OPCARE9.
OPCARE9 generated a series of research protocols for further research and development, which have been taken forward within the Key Research and Development arm of our International Collaborative. A final Dissemination Conference involving over 300 multi-professional delegates worldwide, and a high profile international Policy Summit, presented findings of best practice, key issues, and themes from OPCARE9, which was attended by senior governmental and clinical practitioners from the 9 countries of the project.
To take forward this work it was agreed in November 2013 to establish ‘The International Collaborative for Best Care for the Dying Person’, taking our collaborative of leading international experts and researchers forward in a renewed focus on the international evidence and the next steps in improving care for dying patients and their families. This has strengthened worldwide commitment and capacity to undertake high quality, robust research, to utilise service innovation and improvement methodology, evaluation, and knowledge transfer to improve care for the dying in the 21st Century on a global basis.
The Collaborative was formally launched in January 2014 and its first International Conference was held in Lund, Sweden in November 2014. A constitution was agreed and an executive committee established. The Chair of the Collaborative is John Ellershaw Professor of Palliative Medicine University of Liverpool and the executive committee has representatives from seven countries.
The Objectives of the Collaborative: The collaborative will
Build on, extend, and foster the Collaborative working relationship established during the OPCARE9 EU 7th Framework Project guided by the principles of the Collaborative for Best Care for the Dying Person
Drive forward an international ‘care for the dying’ research agenda and to undertake collaborative international research
Encourage international learning and teaching collaborations to improve the care for the dying
Set, articulate and nurture care for the dying related values, quality indicators, obligations, and strategic aims across the international clinical community
Provide an international platform for health professionals to communicate with each other to improve the care for the dying
To support the development of an “international programme” and associated materials and processes within a five-year Quality Assurance Cycle
Develop an effective communication strategy across international partners to enable innovative growth in support of dynamic international care for the dying work streams acknowledging, disseminating, and celebrating success
Develop and take part in societal debate about care for the dying person and the wider issues of death and dying in society
Hold an Annual General Meeting
Hold an Annual International Conference.
The Work of the Collaborative: The work of the Collaborative incorporates project groups around four main themes:
The International Programme
Research and Development
Learning and Teaching
Quality assurance.
The International Programme incorporates core clinical guidance derived from the International 10 Principles and the International Core Elements for Best Care for the Dying Person[4] that enables effective engagement at the clinical interface supported by a robust implementation and dissemination process for translation of best care to the bedside. This Programme is at the heart of what the Collaborative does.
If member organisations wish, they are free to submit their care plan to the Executive committee for congruence assessment against the Internationally agreed guidance. If congruent the organisation is able to badge their document with the Collaborative logo.
The Research and Development theme incorporates project groups to strengthen worldwide commitment and capacity to undertake high quality, robust research in this complex, critical area of care. This includes a range of cross cutting themes and methodologies including quality outcomes and indicators. The Collaborative will enable valid, reliable and transferable evidence to be generated, supporting important developments and advances in clinical practice and policy. Collaborative partners have recently been successful in securing an ERANET LAC research grant, for a proposal submitted by Professor Dagny Faksvag Haugen from Norway on behalf of the Collaborative. The countries involved in the study are Norway, Germany, Poland, UK, Argentina, Brazil and Uruguay. The investigation focuses on bereaved family's perception of the care for their dying relative received using the Care of the Dying Evaluation (CODE) Questionnaire (Mayland et al. 2014).[5]
Another project group is currently working on the development of a core outcome set for best care for the dying person which is being led by Professor Steffen Eychmueller from the University of Bern Switzerland.
The Learning and Teaching theme incorporates projects groups that serve to articulate, disseminate and evaluate education and training opportunities and collaboration, to develop and nurture a generation of practitioners with the confidence and competence to work within a multi professional dimension, bridging the gaps between science and policy, medicine and health. The Collaborative is looking to establish International Reference Centres to help drive up the education of health care professionals to enable them to implement the Collaborative programme. Nurses within the Collaborative have also set a project group. As the main implementers of the Collaborative programme this group will enable them to share experiences and knowledge as well as giving them mutual support. Cudeca Hospice in Malaga hosts the Summer school in June 2017 for any health care professional wishing to learn about the Collaborative and in particular the different Quality Assurance projects underway, which is the main theme of the summer school. Details can be found on the Collaborative website.
The Quality Assurance theme incorporates project groups to build on our work to date regarding cutting edge real world evidence incorporated into transferable sustainable quality assured processes which will have the capability of improving the quality of life for dying people however and wherever they die. We have developed a Clinical audit tool which is a web-based data entry tool which takes data from individual patients’ case notes; measured against quality statements in keeping with best evidence for care of the dying.
Conclusion: The Collaborative were delighted to welcome the Indian Association of Palliative Care as members in 2014 and very pleased to run the Foundation course at the Bangalore Baptist Hospital, Bangalore, in January 2016. This has resulted in the formation of Project India, a group working together with members of the Collaborative striving to implement an agreed care plan into clinical organizations across India in an effort to drive forward care for the dying person in India.
For anyone wishing further information on the International Collaborative for Best Care for the Dying Person. Please Contact Dr Susie Wilkinson drsusie@btinternet.com
Keywords: Care pathways; end of life care; palliative carel quality assurance
R<sc>EFERENCES</sc>EllershawJWilkinsonSCare of the Dying: A Pathway to Excellence20112nd revised edOxfordOxford University PressCostantiniMRomoliVLeoSDBeccaroMBonoLPilastriPLiverpool care pathway for patients with cancer in hospital: a cluster randomised trialLancet201438322637NeubergerJMore Care Less Pathway: A Review of the Liverpool Care Pathway2013Available from: http://www.gov.ukEllershawJELakhaniMBest care for the dying patientBMJ2013347f4428MaylandCRLeesCGermainAJackBACoxTFMasonSRCaring for those who die at home: the use and validation of ‘Care of the Dying Evaluation’ (CODE) with bereaved relativesBMJ Support Palliat Care20144A40doi:10.1136/bmjspcare-2013-000596Day 2: Plenary 4: What Every Palliative Care Provider Needs to Know about Eolc Legislation in IndiaGursahaniRoopDepartment of Neurology, P. D. Hinduja National Hospital, Mumbai, Maharashtra, India E-mail: roop_gursahani@hotmail.com
EOLC legislation worldwide is a product of the elaboration of the principles of bioethics and simultaneous medical advances in intensive care and transplantation technology through the second half of the 20th century. A major landmark was the Nazi doctors’ trial and the subsequent elaboration of the Nuremberg code on human experimentation in 1947.[1] Through the next two decades improvements in ICU care and widespread availability of artificial ventilation and other life sustaining therapies meant that previously unsalvageable patients could now hope to return to normal life. It also became obvious that not everybody could be salvaged and the first living wills were proposed in the 1960s in the USA. Brain death was first recognized in 1959 both as an artefact of medical technology and as an ethical dilemma. Almost 20 years later, the United States accepted the legal and ethical equivalence of brain and circulatory death. The first edition of Beauchamp and Childress’ seminal text on principles of biomedical ethics was published in 1979.[2] At the turn of the century, the US Patient Self-Determination Act gave shape to the individual right to a natural death.
In India, much of this has passed us by. The Human Organ Transplantation Act recognizes brain death but only for the specific purposes of harvesting organs. The Aruna Shanbaug case is effectively applicable only to the rare cases of persistent vegetative state. Fortunately the judges did go a little further and specifically decriminalized decision making in medical futility. But some constitutional and legal protections for life support limitation were already available as detailed by Mani[3] and it is obvious that the perceived vulnerability of physicians in this regard is overblown.
Nevertheless, India does require comprehensive EOLC legislation to (1) provide legal validity to advance care planning, directives and health care power-of attorney; (2) create transparent and viable processes for determination of medical futility and withdrawal/withholding of life sustaining therapies; (3) recognize the equivalence of brain and circulatory death. In 2015, three national medical associations of intensivists, neurologists and palliative care physicians came together to draft such a law. This has been done and this law is now due for release in the public domain. But the law alone is not enough. The issues that make EOLC both crucial and difficult need widespread public awareness and discussion. We also need wider access to generalist palliative care by training family physicians, internists and other medical specialties in the basic principles of palliative care. It is thus extremely important for Palliative Care Physicians across the country to come together to push for this law, to work together to increase public awareness of these issues and to educate the wider medical community in generalist palliative care.
Keywords: Ethics; end of life care legislation; life support limitation; palliative care
R<sc>EFERENCES</sc>ShusterEFifty years later: the significance of the Nuremberg CodeN Engl J Med1997337143640RauprichOVollmannJ30 years principles of biomedical ethics: introduction to a symposium on the 6th edition of Tom L Beauchamp and James F Childress’ seminal workJ Med Ethics2011375823ManiRKConstitutional and legal protection for life support limitation in IndiaIndian J Palliat Care20152125861Day 2: Plenary 5: Palliative Care and Humanitarian AidSuttonBrettDepartment of Health and Human Services, Melbourne, Victoria, Australia E-mail: Brett.Sutton@dhhs.vic.gov.au
Over 87 million people across 37 countries are expected to require life-saving humanitarian assistance in 2016. Amongst them, refugees and other displaced individuals (12.4 million newly displaced in 2015 stand at the forefront of global institutional and individual citizens’ concern. According to the United Nations (UN) High Commissioner for Refugees 2014 report, nearly 60 million people were forcibly displaced worldwide by wars, conflict and persecution alone.
The need for a common multi-faceted framework including the health sector has been clearly recognized in responses to the migration crisis. Palliative care, however, has been largely omitted from this emergency specifically and humanitarian crises generally. Palliative care is “an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering”. Its omission from humanitarian responses contradicts the World Health Assembly's acknowledgement that palliative care is an ethical responsibility of health systems that should be available to all and leaves millions of disaster victims with preventable suffering. We propose that palliative care should be an integral component of relief strategies; a new component of disaster planning.
Palliative care is especially applicable in the following humanitarian scenarios: (i) in protracted humanitarian crises, for patients with life-limiting illnesses who have either been receiving palliative care before the crisis and experience interruption in that care, or who have had unmet palliative care needs before the crisis, potentially exacerbated as a result of it; (ii) in the context of mass casualty events, where the death toll is high, resources are overwhelmed by casualties with injuries of variable severity, and individuals are triaged according to their likelihood of survival; (iii) in communicable disease outbreaks with high mortality and limited therapeutic interventions, where the relief of suffering can be the only treatment option available, as was the case with Ebola; (iv) in refugee and displaced persons camps, where a proportion of individuals will require palliative care during a potentially brief period of transition through the camp.
No formal measures exist of the extent of suffering during such crises, including the number of individuals who could benefit from palliative and end-of-life care. The reference point for deaths in the UK under ‘normal’ circumstances is one percent of the population. Clearly, there are crises where the percentage of people requiring palliative and end-of-life care would be far greater than that. Reliable estimates are urgently needed.
Triage systems in humanitarian settings, particularly in acute ones, have low sensitivity to the need for palliative care. Originating in the work of Surgeon Marshal Baron Dominique Jean Larrey during the Napoleonic Wars, the initial aims of triage were militaristic. The highest priority was accorded to soldiers with minor wounds who could return to the battlefield with minimal treatment. Latterly, triage has become a daily management tool within civilian emergency departments with the utilitarian aim of doing “the most for the most” when casualties’ needs exceed the capacity of immediately available skilled help.
Mass casualty, as opposed to routine clinical, triage is therefore predicated on the notion that care provided to those with unsurvivable injuries is an unreasonable use of resources. In these settings the narrative is focused on the ‘realm of the possible’. Palliative care, in contrast, tends to be relegated to the domain of the infeasible or impossible, allowing preventable suffering to occur.
In addition to deprioritizing the suffering of those likely to die, current triage systems used in humanitarian contexts may, in fact, exacerbate it. The Triage Revised Trauma Score, for instance, applies a threshold that can direct patients with a survival probability of under 50% to life-saving care. As a result, many may receive unnecessary invasive and intensive ‘life-saving’ procedures, which are not only futile, but also cause suffering and loss of dignity. Additionally, staff and witnesses may be traumatized by their unsuccessful attempts to resuscitate an expectant patient. The provision of basic palliative care as an alternative for appropriate patients is, by comparison, relatively simple without requiring significant resourcing. Indeed, much care can be provided by family and loved ones with access to essential medicines, guidance and training.
Palliative care provision in disaster settings is also vulnerable to rapid evacuation needs, which can lead to patients being left unattended or subject to euthanasia proposals. The latter were the focus of inquiry in the US after Hurricane Katrina, when a physician in New Orleans euthanized patients who could not be evacuated from a critical-care unit. Even where immediacy is not a pressing consideration, palliation is still often neglected. For example, during the Ebola crisis, palliative and supportive measures were essential care elements which could have been systematically implemented. Mortality approached 90% for infected infants, yet no indication exists that palliative specialists were recruited or formally consulted.
Given the relatively recent development of palliative care, it is timely to ask if the standard humanitarian response of saving lives to minimize suffering should be re-imagined as a paradigm of saving lives and minimizing suffering. This is a critical distinction. If we agree with the latter conceptualization, palliative care – care for individuals who may not recover from their life-limiting illnesses/injuries – must be recognized as an incontestable part of a larger holistic reaction to such crises.
Existing standards of clinical care for crisis settings emphasize that dying patients should be treated with respect, accompanied, provided with pain relief and have other severe symptoms relieved to help ensure dying is as comfortable and meaningful as possible. Moreover, the Humanitarian Charter of the Sphere Handbook, the pre-eminent global guidance in humanitarian disasters, explicitly references the common rights of affected populations, including: the right to life with dignity; the right to receive humanitarian assistance; and the right to protection and security. 26 Providing palliative care is a means of upholding all three without neglecting the imperative to save lives.
It seems that palliative care is often perceived as a poorly prioritized end-of-life intervention that applies exclusively when all curative treatments are redundant, when there is “nothing left to offer”, rather than as intended to minimize patients’ suffering and maximize their quality of life.
The relative absence of specific palliative care guidance in humanitarian standards also precludes humanitarian workers from applying consistently good practices when faced with palliative and end-of-life care needs. They may be unsure what to do or have insufficient resources for minimum standards of care. This is especially the case for essential medicines – such as highly affordable oral morphine – resulting in ineffective pain management or, at worst, treating patients as if they are already deceased. Palliative care standards should include, at the very least: minimum training requirements for all humanitarian health workers; the addition of essential medicines for palliation into medications kits; guidance and tools on essential palliative care practices; and recommendations for creating a supportive policy environment. Humanitarian organizations and palliative care practitioners need to work closely together to find feasible mechanisms to bring palliative care into mainstream humanitarian health practices. The research and information void on the topic also needs to be urgently addressed.
Lastly, whilst being debated by UN human rights treaty bodies, state obligations during natural or human-made catastrophes are unclear. In particular, there is no consensus on the minimum requirements to living a dignified life that should be guaranteed to everyone at all times.
The palliative care community must unite to offer workable and sustainable solutions in conjunction with humanitarian partners as part of an integrated disaster response package. In addition to saving lives, the relief of suffering in the dying and severely ill must be enabled during a humanitarian response.
Keywords: End of life care; humanitarian aid; humanitarian emergency; minimum standards; suffering; SPHERE
Day 3: Plenary 7: Chronic Sorrow: A Path Less TravelledAndersonKarenDepartment of Counselling and Psychotherapy, School of Arts and Humanities, Edith Cowan University, WA, Australia E-mail: karen.anderson@ecu.edu.au
Whilst grief, loss and bereavement are all integral to working in palliative care and impact across disciplines the concept of chronic sorrow has received less consideration until more recently. Originally termed in the early 1960's to address the relentless sense of loss experienced by parents following a diagnosis of a child's intellectual or other severe developmental disability the concept is now being viewed as applicable to chronic and terminal illnesses. Where there are periodic recurrences of permanent and pervasive sadness chronic sorrow may exist. Chronic sorrow differs from major depression and depressive disorders which are usually associated with habitual, self-critical patterns of thinking. With chronic sorrow the level of functioning remains reasonably stable. A person experiencing chronic sorrow will often detect when they are moving towards becoming depressed and will acknowledged they’re feeling ‘burnt out’. This instigates making adaptations so as to extract further strength and stamina to continue to step through the challenges life presents. Hence, there exists a sense of some days being good and satisfying whilst other days are exhausting, threatening and even traumatic.
The presentation will elaborate on the historical and recent contexts for applying the concept of chronic sorrow as well as define the term. Understandings of various aspects and considerations of chronic sorrow will be included. Relevance for incorporating improved awareness of the concept of chronic sorrow into palliative care work is encouraged.
Keywords: Chronic sorrow; palliative care; self care
Day 3: Plenary 8: The Philosophical and Cultural Situatedness of Spirituality at the End of Life in IndiaInbadasHamiltonResearch Associate, School of Interdisciplinary Studies, The University of Glasgow, Dumfries, Scotland, UK E-mail: Hamilton.Inbadas@glasgow.ac.uk
The sustained interest in exploring the spiritual domain at end of life in the Indian context reflects the recognition of its significance as an aspect of palliative care. Several studies have sought to explore this critical end of life zone. There have been quantitative studies aimed at the effectiveness of attention to spirituality and spiritual care at the end of life and qualitative studies that explored the features of spirituality based on the experiences of patients and perceptions of professionals.[1234]
A key aspect of the findings from studies so far is the recognition and identification of challenges, inadequacies, limitations and ethical dilemmas in relation to spirituality at the end of life. These are also often reflected in commentaries and are part of presentations at scientific meetings. There has been a genuine sense of inadequacy that we do not know what spirituality at the end of life means.[5] The existence of many religions and the fact that health care professionals and care receivers can have different religious affiliations has been perceived as a challenging context in India.[6] In a country where access to basic palliative care and pain medicines are scarce, the sense of inadequacy of personal and financial resources is overwhelming. In addition, a recent systematic review of studies on spirituality at the end of life in India highlighted fundamental ethical challenges in providing spiritual care in the Indian palliative care setting.[7] Many of these have identified features that are culturally characteristic of the Indian way of life; particularly making reference to the significance of religious faith for most of the Indian population and the importance of family and community. However, an in-depth exposition of religious, philosophical and cultural tenets to inform our understanding of spirituality and spiritual care is lacking.[8]
India is known for its rich spiritual heritage and has unique ways of understanding, experiencing and expressing spirituality. The philosophical and cultural frames of reference, with which communities in India make sense of life, death and dying, determine the characteristics of Indian spirituality at the end of life. In international literature, spirituality is often characterised as the ‘essence of the human person’ and the ‘meaning and purpose of life’.[910] These are philosophical concepts that shape our perceptions of our identity and our experience of living in human communities in particular contexts. Similarly, ‘death’ is not only an event of life but also carries with it considerable philosophical and cultural concepts that gives meaning to death and the experience of dying.
Communities around the world have been responding to end of life issues in different ways and some have focused their efforts on ‘intangible’ aspects of care provided at the end of life, such as spiritual care.[11] Drawing ideas and methods from different parts of the world to address end of life issues is an increasingly common phenomenon in the contemporary world.[12] While this can potentially facilitate mutual learning, it also accounts for the lack of attention to the particularities of the local context. Drawing ideas and concepts from elsewhere may provide some guidance, however, it undermines the possibility of creating a knowledge base informed by philosophical, theological and sociological concepts, which are critical to the understanding of spirituality.
Critical differences between Indian philosophical approaches and others, particularly those of the Western world have been well established. Indian philosophy engages with metaphysical questions arising from the experiences of life where the divine and the human share in the formation of understanding, with direct implications to practical everyday life (Sādhanāe).[1314] Exploring the concepts of the human person, the purpose of human life, the meaning of death and caring for the dying using Indian philosophical and cultural resources, therefore, offers the opportunity to understand the unique ways in which they shape the Indian understanding and experience of spirituality at the end of life.
The concept of the human person is based on the understanding that the human soul is from the divine and is of the same substance as its divine source. It is not the individual's capacity as a ‘thinking being’ or a ‘rational being’ that gives the human person his/her existence. It is an extension of the divine, a gift of God. The purpose of life is the ultimate liberation from the māya of this world and to be united with the divine.[15] Following the right way of life, discerning the will of God and following it is central to the understanding of the purpose of life.[1617] It is significant to recognise that purpose of life in the Indian conscience is not individually thought out and self-determined. Following on from the two former concepts, death is understood as a process, a passage, rather than a termination of existence.[18] In the words of Rabindranath Tagore, “Death is not extinguishing the light; it is only putting out the lamp because the dawn has come.”[19]
A study exploring a historical-cultural understanding of spirituality in India, identified ‘Union with the divine’, ‘being at peace’ and ‘preserving dignity’ as the three core principles of spirituality at the end of life in India.[20] These principles were found to be at the heart of the practices and beliefs in the context of the care of the dying. For example: ‘a daughter's wedding’ is a common cause of worry for many palliative care patients. It sounds reasonable that this can be understood as ‘unfinished business’ and classified as a ‘social’ aspect of the total pain the person is experiencing. But viewed through the Indian philosophical and cultural lens, it can be understood in a deep spiritual way. A daughter's marriage is not merely ‘unfinished business’ - a special occasion in the family and an important event in the life of the daughter, which the parent likes to witness before s/he dies; the worry stems from a deep sense of responsibility as a parent, an identity which has embedded in itself the moral duty to make sure his/her daughter is settled in life. Deliverance from this bondage to the sense of duty leads to the opportunity of dying in peace; and in dignity, with the realisation of the divine within oneself; and with only ‘God-thought’ at the time of death, leading to union with the divine.
Cultural aspects are particularly important while considering models of spiritual care. Other than the new Christian mission hospitals in India, the idea of a chaplain is an unfamiliar concept.[21] Professional spiritual care providers are not part of India's health care fabric. It is widely held, particularly among palliative care communities, that ‘being with’ and ‘listening’ are essential skills all palliative care professionals should exercise to provide spiritual care for their patients and families.[22] While there is no doubt that patients greatly benefit from the presence and the listening of health care providers, which can lead to spiritual healing, it cannot be ignored that emphasis on these skills assumes that the patient is able to think through, rationalise and articulate their spiritual experiences. The words they say and the observations of the professional become the basis for assessing spiritual needs. This may be in conflict with the Indian sense of spirituality, where people often find practices and experiences deeply meaningful, but are not always are able to describe or explain it. Spirituality therefore remains something people experience as being someone, being part of something significant and doing something that is meaningful for them, though they may never find the words to describe their experience.
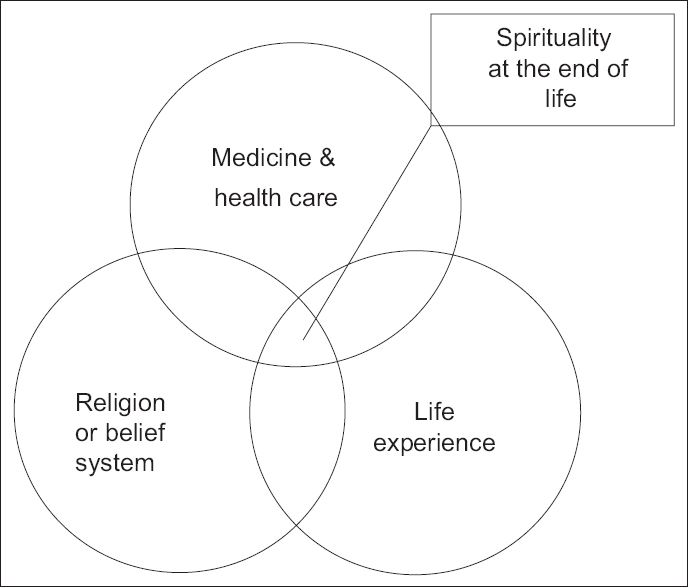
Spirituality at the end of life can be conceptually seen as the area of common overlap of three domains [Figure 1]. The life experience of people and organised religion or belief system form the first two domains. In ordinary circumstances of life people constantly draw, experience and interpret spiritual meanings from their affiliation to religion or a belief system. In the context of end of life care, the domain of medicine and health care gets to be an influential factor. Much of the search for understanding spirituality seems to remain within the narrow triangle of the area of common overlap of the three domains, often drawing tools and methods used in medicine and health sciences. There is little engagement with the domain of religion and belief systems that accounts for spiritual meanings and experiences for the rest of people's lives.
Spirituality at the end of life
‘How to recognise spiritual distress at the end of life?’ is a question frequently voiced in palliative care meetings. How do we recognise spiritual distress in ordinary circumstances, in non-end-of-life situations? Responses to this question might have implications for how we recognise and respond to spiritual distress in palliative care. and more importantly, such answers cannot be found if we keep looking inside the little triangle using tools from the medical domain. We need other approaches, such as theology and philosophy that have expertise in the domain of religion and belief systems and sociology and psychology with their resources to make sense of the life experiences, to help us see the whole picture.
A cross-disciplinary approach, drawing together expertise from clinical palliative care, philosophy, theology and sociology, will enrich the understanding of spirituality at the end of life and can contribute effective means of providing spiritual care in palliative care in specific contexts around the world.
Keywords: end of life care; human person; Indian spirituality
R<sc>EFERENCES</sc>ShuklaPRishiPA corelational study of psychosocial & spiritual well being and death anxiety among advanced stage cancer patientsAm J Appl Psychol201425965KandasamyAChaturvediSKDesaiGSpirituality, distress, depression, anxiety, and quality of life in patients with advanced cancerIndian J Cancer201148559LoiselleCGSterlingMMViews on death and dying among health care workers in an Indian cancer care hospice: balancing individual and collective perspectivesPalliat Med2012262506SimhaSNobleSChaturvediSKSpiritual concerns in Hindu cancer patients undergoing palliative care: a qualitative studyIndian J Palliat Care20131999105RajagopalMPain and beyondIndian J Palliat Care20061247ShubhaREnd-of-life care in the Indian context: The need for cultural sensitivityIndian J Palliat Care2007135964GielenJBhatnagarSChaturvediSKSpirituality as an ethical challenge in Indian palliative care: A systematic reviewPalliat Support Care20161456182InbadasHHistory, culture and traditions: The silent spaces in the study of spirituality at the end of lifeReligions2016753FeggMJBrandstätterMKramerMKöglerMHaarmann-DoetkotteSBorasioGDMeaning in life in palliative care patientsJ Pain Symptom Manage2010405029WrightMPayneSSeymourJIngletonCGood for the soul? The spiritual dimension of hospice and palliative carePalliative Care Nursing: Principles and Evidence for Practice2008BerkshireOpen University Press21231ClarkDZamanSInbadasHWhitelawAInterventions at the end of life: A taxonomy and critiqueManuscript in Preparation2016ZamanSInbadasHWhitelawAClarkDCommon or multiple futures for end of life care around the world? Ideas from the ‘waiting room of history’Soc Sci Med2017172729GaneriJThe Concealed Art of the Soul: Theories of Self and Practices of Truth in Indian Ethics and Epistemology2007New YorkOxford University PressHiriyannaMThe Essentials of Indian Philosophy1995New DelhiMotilal Banarsidass PublVivekanandaSThe Complete Work of Swami Vivekananda19912CalcuttaAdvaita AshramaKonwarBVivekananda's concept of karmaSoc Sci Res201321621MohantyJNIndian Philosophy2001New DelhiOxford University PressAdikalaarKReligion and Society in Our View1975ChennaiChennai UniversityMajdiSThe Wisdom of the Great2012BloomingtonUniverse, IncInbadasHSeymourJNarayanasamyAPrinciples of spiritual care in end-of-life care in India: A historical-cultural investigationBMJ Support Palliat Care20144Suppl 1A18EdasseryDKuttierathSSpirituality in the secular senseEuro J Palliat Care19985165LunnJSSpiritual care in a multi-religious setting revisitedIndian J Palliat Care200713657Day 1: Hall A, 11 Am to 12 Am: High Fives on Pain: MethadoneHardyJanetMater Health Services Center, Mater Research University, Queensland, Australia E-mail: janet.Hardy@mater.org.au
Methadone – is this a special opioid?: Methadone was first synthesised over 60 years ago. It has gone in and out of ‘vogue” over the years but has had a recent resurgence in popularity because of its perceived benefit over other opioids in difficult pain scenarios, especially in neuropathic pain.
Because of its unique pharmacokinetic and pharmacodynamics properties, methadone can be very difficult to use and can lead to unexpected toxicity. It carries the stigma of being the drug used in opioid addiction programs.
It has a number of advantages including a long half-life, an elimination pathway independent of renal function, lack of active metabolites, high oral bioavailability and cheap cost.
Disadvantages include difficulties in titration and conversion from other opioids, marked inter-individual variability in dose and efficacy and a significant risk of toxicity.
There are many published regimens for conversion to methadone in the context of opioid rotation. Different schema result in marked variation in dose and there is no evidence to support any one method over another. Many prefer to use methadone as an adjuvant, in conjunction with other opioids. Although considered a “special opioid”, there is very little evidence of benefit over other opioids in efficacy or toxicity. Despite this, there is anecdotal evidence of benefit in situations where other opioids have failed to give adequate pain relief.
Keywords: Cancer pain management; methadone; opioids
Day 1: Hall A, 11 Am to 12 Am: High Fives on Pain: Opioids for Nonmalignant PainReddySuresh KUniversity of Texas MD Anderson Cancer Center, Houston, Texas, US E-mail: sreddy@mdanderson.org
The number of patients suffering from chronic non-malignant pain in India is unknown, but the incidence is likely to go up due to increase in non-communicable diseases. Over the last few decades India witnessed rapid Industrialisation. It is likely that the incidence of osteoarthritis, pain syndromes like chronic back pain, chronic neck pain, and chronic headaches are likely to increase over the next few decades. Other non-malignant entities which results in moderate to severe pain include peripheral vascular diseases, diabetic related neuropathy and chronic pancreatitis. In addition, HIV and AIDs results in chronic pain syndromes at multiple locations of varying intensities [Table 1]. All these syndromes are generally associated and influenced by psychosocial elements. Optimal assessment and management of these pain syndromes will help in improving quality of life and preventing loss of work productivity. The treatment of non-malignant pain syndromes is generally aimed at treating the cause, improving function and quality of life. The goal and focus should be on improving function and return to work. Management of pain includes both pharmacological and non-pharmacological interventions. During 90s, the use of opioids for cancer pain had increased exponentially. The outcomes in cancer pain encouraged physicians to use opioids in non-malignant pain using the same algorithms with suboptimal risk assessment. Pharmaceutical companies provided the marketing catalyst and encouraged physicians to prescribe opioids for non-malignant pain syndromes. Now US is witnessing an epidemic in prescription abuse of opioids. Current evidence do not support the use of opioids in non-malignant pain[123]. However in individual cases one must balance the risks and benefits. One must Identify goals, high risk individuals, and adopt a rehabilitation approach. Recently, the Center for Disease Control issued newer guidelines and check list on opioid use in non-malignant pain[4].
Non-malignant pain syndromes
Keywords: Abuse potential; chronic non malignant pain; opioids
R<sc>EFERENCES</sc>FurlanADSandovalJAMailis-GagnonATunksEOpioids for chronic noncancer pain: a meta-analysis of effectiveness and side effectsCMAJ2006174158994ChouRBallantyneJCFanciulloGJFinePGMiaskowskiCResearch gaps on use of opioids for chronic noncancer pain: findings from a review of the evidence for an American Pain Society and American Academy of Pain Medicine clinical practice guidelineJ Pain20091014759Von KorffMKolodnyADeyoRAChouRLong-term opioid therapy reconsideredAnn Intern Med20111553258DowellDHaegerichTMRogerCCDC Guideline for prescribing opioids for chronic pain-United States MMWR Recomm Rep 2016:65(No.RR-1)149Day 1: Hall B, 11 Am to 12 Am: Education in Palliative Care: Global Education Program: Palliative Care Always: Massive Open Online Education to Build Primary Palliative Care in a Global AudienceRamchandranKavitha12TribettErika12ChanSandy12FronkJoshua12PassagliaJudy12BugosKelly12SicklerKim12KleinLori12KogonManuela12HuttonLynn12BrownEllen12LyoGrace12SledgeGeorge12Division of Oncology, Stanford University, California, USADivision of General Medicine Principles, Stanford University, California, USA E-mail: kavitha@stanford.edu
Background: Primary palliative care (PC) is critical to improve access to PC from the point of diagnosis. Still, barriers exist to providing primary PC worldwide, including a lack of awareness, time, and training. Interactive online learning experiences can help overcome these. This project describes a massive open online course (MOOC)-Palliative Care Always-designed to build primary PC skills in a global audience.
Methods: A team of PC providers and online instructional experts developed 12 modules that included: (1) patient scenes, (2) brief lectures, (3) empathy exercises, and (4) Google Hangout discussions. Course objectives included awareness of PC, practicing effective communication skills, basic symptom assessment and management. The target audience included oncology clinicians from a variety of disciplines; secondary audience included patients and families. The MOOC launched January-April 2016. Participant engagement, satisfaction and self-reported knowledge were assessed through pre- and post-surveys. Multiple choice assessments captured knowledge gain. Follow-up assessments will be distributed three months post-MOOC.
Results: By April 2016, the course reached 1,420 participants from 91 countries. 54% were from the US, followed by India, Brazil, and Canada. 76% were healthcare professionals, the majority being nurses (40%), physicians (19%) and social workers (13%). The remaining 24% included patient, caregivers, and others interested in PC. Top reasons for enrolling were interest in PC, personal growth and job relevance. On average, 27% of enrollees actively engaged week-over-week. Eighty-six percent of respondents were “very satisfied” with the amount learned, and over 50% cited learning “a great deal” in: communicating difficult news, goals of care, psychosocial and hospice care. Respondents desire additional content related to: caregiver experience, advanced symptom management, and points of conflict in treatment plans. 93% cited being “very likely” to recommend the course.
Conclusions: Interactive MOOC experiences have the potential to build PC awareness, primary skills and global PC networks. Upcoming iterations will incorporate: accommodations for varying levels of PC knowledge; additional opportunities for interaction between participants, including social networks; blended learning; and evaluation of impact on practice and healthcare outcomes.
Keywords: Blended learning; global palliative care; MOOC education
Day 1: Hall A, 12 Pm to 1 Pm: High Fives on Other Symptoms: Delirium: Applying Recent Evidence for Better Delirium Care at the End of LifeAgarMeeraDepartment of Palliative Medicine, Centre for Cardiovascular and Chronic Care, University of Technology Sydney and Sydney South West Clinical School, University of New South Wales E-mail: Meera.Agar@uts.edu.au
Delirium is a prevalent syndrome in palliative care, associated with significant distress for patients and their caregivers. This talk will address the clinical challenges of delirium in palliative care, provide updates on the relevant literature from the last five years to inform prevention, screening, detection, risk factors and management; and provide comment on implications for clinical practice and research. The implications for communication, clinical decision-making and support for families witnessing delirium will also be discussed.
In particularly it will address:
What is the latest understanding of delirium pathophysiology?
What do we understand about delirium epidemiology in palliative care?
What are the factors that predispose and precipitate delirium in advanced illness and how reversible are they?
Can we prevent delirium in patients with advanced illness or cancer?
How does the current evidence for delirium pharmacological and non-pharmacological management inform care for the person with advanced disease?
What is the impact of delirium on the person's loved ones and implications for grief and loss.
Keywords: Delirium; end of life care; non-pharmacological treatment; pharmacological treatment
Day 1: Hall B, 12 Pm to 1 Pm: Taking Care of Children: Children with HIVDowningJuliaHonorary Professor, Makerere University, Kampala, Director of Education and Research for International Children's Palliative Care Network E-mail: julia.downing@icpcn.org
The HIV epidemic varies in different parts of the world, with some areas having a significant number of children with HIV who need palliative care. India has the 3rd largest HIV epidemic in the world with around 2.4 million people living with HIV and children account for 3.5% of all infections. There are approximately 19,000 new infections in children a year, and only 41% of those children needing ART access it. Palliative care is an essential component of the comprehensive package of care for children living with HIV/AIDS from diagnosis into advanced AIDS, end-of-life care and bereavement. A multi-sectoral approach to care is required with an emphasis on primary care, as most children are managed at the primary care level.
This presentation will discuss the impact of HIV on children and the uncertain progression of the disease with high levels of morbidity and mortality. The principles of palliative care for children with HIV which includes multi-disciplinary family centered care, and focuses on the higher burden of physical, psychological and spiritual needs experienced by children with HIV & AIDS is essential. In addressing this, the pathology of HIV will be discussed along with pain and symptom management, psychosocial care, spiritual care and the integration of palliative care with ART in children. HIV impacts the whole family this family-centered care is essential along with care in the primary health care setting. Palliative care for children with HIV and their families therefore remains an essential component of HIV care provision.
Keywords: End of life care, HIC/AIDS; paediatric palliative care
Day 1: Hall B, 12 Pm to 1 Pm: Taking Care of Children: Empowering Bereaved ParentsDeodharJayitaDepartment of Palliative Medicine, Tata Memorial Hospital, Mumbai, Maharashtra, India E-mail: jukd2000@yahoo.co.uk
The death of a child is one of the most stressful experiences for the parents, impacting on their physical and psychological health, and increasing risk for mortality. The main interventions used are support groups (self-help or facilitator led), counselling, psychotherapy and pharmacotherapy (for mainly depressive episodes). The evidence for these interventions, as reported in a systematic review, is of low quality. Helping parents to cope and gain some control over a despairing view of the present and future needs intense, well-integrated and interdisciplinary approach. Components derived from the aforementioned interventions can prove helpful. Parents need bereavement specific programmes which can suit their needs for support, sharing, advice, practical help and information. These programmes need to be flexible and available at any point in the parents’ grief journey. Developing peer support has been found to be useful, both for the parents who are receiving and giving support, with a addition of a ‘mentorship’ value. Having a volunteer who supports the parents when child is diagnosed as terminally ill, during bereavement and for a year after the death of the child has also been found useful. Giving an opportunity to the bereaved parents to decide what would be helpful for resources for information and/or therapy for themselves and their peers can give them ownership of the programme. Also, involving them in educational programmes for palliative care by sharing their real life stories can be cathartic for them and help others learn through their experience. In my personal experience, once the bereaved parents have worked through their grief, they have joined as volunteers in the paediatric oncology service, and are an invaluable support for other parents of sick children. Inclusion of bereaved parents in guiding and developing appropriate programs can be the way forward for empowering bereaved parents.
Keywords: Bereavement; bereaved parents; grief
Day 1: Hall B, 12 Pm to 1 Pm: Taking Care of Children: Spiritual Needs of Children: Spirituality in Pediatric Palliative Care: Practical and Ethical Considerations for the Indian ContextGielenJorisCentre for Health Care and Ethics, Duquesne University, Pittsburgh, USA E-mail: gielenj@duq.edu
In palliative care literature, spirituality is generally recognized as an important aspect of holistic care. Data indeed show that many patients at the end of life have specific spiritual needs that have to be addressed by an interdisciplinary palliative care team. Data among adult palliative care patients in India have shown that a substantial proportion of them suffer from spiritual distress. Children have been found to have specific spiritual needs at the end of life, too. However, providing effective spiritual care to children is even more complicated than to adults, because, as children age, they develop physically, emotionally, intellectually, and also spiritually. Their understanding of death develops as well. However, by age seven a majority of children understand the main components of death (universality, causality, irreversibility, and non functionality). These observations lead us to two important conclusions. First, spiritual care has to be tailored to the developmental level of each individual child. Second, given children's early understanding of death, in spiritual history taking there should be an openness from the side of the clinicians to discuss death and dying and how the child relates to these spiritually. In order to enable such a fruitful discussion it is necessary to see the child as an active participant in the care process, and not as a mere recipient of care. This implies that at an age and development appropriate level children should be informed about diagnosis and prognosis and involved in decision-making. Parents, particularly in the Indian context, may object to such involvement, even in the case of adolescents, out of fear for possible harm to their child caused by knowledge of their disease. In such a case, parents should be educated by the team about the need to involve the child in order to enable the best possible care.
Day 1: Hall A, 4.30 Pm to 5.30 Pm: Psychological Issues in Palliative Care: Couples with Cancer: Couples Dealing with Cancer: You, Me and USAndersonKarenSchool of Arts and Humanities, Edith Cowan University, Perth, Western Australia, Australia E-mail: karen.anderson@ecu.edu.au
”When part of the matrix of the relationship is put to the side in order to deal with the cancer and the threat to life and our known existence, the dynamics in the relationship alter and change.” (D.C., client and husband, 2008).
The aim of this presentation is to briefly outline a ‘multiple couples’ model of psycho-social-educational group intervention designed specifically for couples wherein one, or both partners are dealing with a cancer diagnosis. The ‘multiple couples’ model is used to focus support upon the relational basis for meeting the challenge of cancer together as partners (i.e. as a united team) throughout the trajectory of the illness. A diagnosis of cancer, the necessary treatment regime and resultant recovery phase is a significantly stressful event for an individual person, their spouse/partner and their families. When a partner is diagnosed with a life threatening illness such as cancer, it can strain the relationship as roles and needs change. Navigating the terrain in life after a cancer diagnosis individually and collectively as partners, often impacts on the relational resources available in normative couple functioning.
Facing the ‘threat’ presented by cancer is framed as a conjoint issue. Being united as a couple means there is allowance for, and inclusiveness of different views, perspectives and experiences being held by each partner. Existential conversations occur within this couples and cancer framework wherein interactions with other couples have been found to be enabling and useful.
This powerpoint presentation refers to six weekend workshops, conducted over five years and involving 51 couples. Workshop couples’ feedback is used to indicate the viability for further developing the ‘multiple couples’ model to support couples dealing with cancer.
Keywords: Couples therapy; psychotherapy; psychological issues; cancer
Day 1: Hall A, 4.30 Pm to 5.30 Pm: Psychological Issues in Palliative Care: Self Care of the CarerMathewAnjuDepartment of Psychiatry, Government Medical College, Thiruvananthapuram, Kerala, India E-mail: anjumathew2222@gmail.com
Physical and emotional exhaustion, caused by caring for the severely ill, is well known in the field of Palliative Medicine. The Carers, including the family, friends and health professionals are at a high risk for burnout, psychological distress and compassion fatigue. The impact of these factors on personal and professional well being will be discussed. Self care enables better caring for the patients in a sustainable way with greater empathy and effectiveness. Strategies to improve self care of the carer, leading to better quality of life of both the patient and the carer, will be discussed in detail.
Keywords: Burnout; carers; self care
Day 1: Hall B, 4.30 Pm to 5.30 Pm: Diversity of Healthcare in India and Integration of Palliative Care Across the Spectrum – In Rural North India in the Community: A Panel Discussion: Model of Palliative Care Delivery in Rural Communities in North IndiaThyleAnnDepartment of Palliative Medicine, Emmanuel Hospital Association, New Delhi, India E-mail: annthyle@gmail.com
Background: EHA's 20 hospitals in 14 north Indian states, provides affordable quality medical and palliative care to the rural poor at remote locations. Cultural attitudes, low literacy rates, inability to access care, lack of knowledge, and crushing poverty results in unimaginable suffering.
Method: Palliative care was recognized as a huge unmet need in rural areas where suffering is intensified from late presentations and limited treatment options. Our objective was to establish palliative home-based, outpatient and inpatient care, accessibility to opioids, ongoing training for teams, families and primary health care providers; also prevention, early detection and treatment programmes, with measures for income generation and household poverty alleviation.
Methodology: Palliative care services were established at 9 rural hospitals located in U.P, M.P, Assam, Bihar, Maharashtra and Jharkhand, and 1 in Delhi for the urban poor. Mapping of palliative care needs revealed the full spectrum of life-limiting illnesses. Home care services by trained teams were set up, backed by outpatient and inpatient facilities. Awareness-raising targeted health professionals, village leaders, communities and carers. The continuum of care included prevention, early detection and treatment options, care packages, children's education support, income generation projects, and advice for Government subsidies. Review, evaluation and recommendations by external experts were implemented.
Results: The rural poor benefited immensely. Enrolment in home care services reduced expenses on medicines, travel and end-of-life care. Narcotics licenses obtained at 4 hospitals. Supportive care allowed family members to continue working. Local Government functionaries, primary health care providers and communities became aware of the scope of palliative care, thus embracing partnerships. Information about government benefits and help with requisite forms allowed access to Government subsidies. Skill development and income generation projects helped contain household poverty.
Conclusion: Providing a continuum of palliative care alleviates suffering in neglected north Indian Rural populations, meaningfully engages stakeholders, fulfils unmet needs, and is a replicable model especially for remote locations.
Keywords: Home based care, North India, poverty, rural
Day 1: Hall C, 4.30 Pm to 5.30 Pm: Palliative Care in Degenerating Neurological Disorders: A Neurologist's PerspectiveAlladiSuvarnaDepartment of Neurology, National Institute of Mental Health and Neurosciences, Bengaluru, Karnataka, India E-mail: alladisuvarna@hotmail.com
Neurological disorders pose unique problems related to management due to their longstanding course, complex and often severe morbidity. Neurological disorders that require palliative care range from diseases with an acute insult and severe residual morbidity to progressive degenerative diseases that have evolving morbidity and needs over years. Management requires the expertise of neurologists and rehabilitation experts to focus on building/retaining/optimising ability in the face of disease progression, as well as palliative care specialists, with significant overlap in their roles. A huge burden of disease coupled with a lack of awareness, training and resources compounds the problem of palliative care in India. The main aim of palliative care is to improve quality of life of patients with chronic neurological disability, and involves several strategies that include person centered care, setting care goals and advance planning, continuity of care, prognostication and timely recognition of dying, optimum symptomatic treatment, psychological support and family care. Education of health care teams is crucial and social and ethical issues need to be addressed and can often be challenging. The need for developing guidelines that are relevant for Indian context will require systematic studies conducted across different disease populations and across sociodemographic strata, so palliative care needs can be identified and service development may be prioritised.
Keywords: Degenerative neurological diseases; Indian health care; palliative care
Day 1: Hall C, 4.30 Pm to 5.30 Pm: Palliative Care in Degenerating Neurological Disorders: Symptom Management in Palliative CareDouglasCarol12Palliative and Supportive Care Service, Royal Brisbane and Women's Hospital, Queensland, AustralianAustralian and New Zealand Society of Palliative Medicine, Australia E-mail: caza87@optusnet.com.au
Motor Neurone Disease or Amyotrophic Lateral Sclerosis requires meticulous attention to symptom management. The rapid trajectory to dying in most patients over short years mandates focusing on quality of life from diagnosis through expert palliation.
Other conditions such as Alzheimer's, Parkinson's and Huntington's Disease progress slowly and may require episodic support by Palliative Care clinicians with increasing support towards the end of life.
There are a number of key symptoms to address with Motor Neurone Disease, including dyspnoea, dysphagia, dysarthria, musculoskeletal pain and cramps, constipation, drooling, emotional lability and psychological distress. A multidisciplinary team approach to care is required to provide maximal support to the patient in addressing these clinical issues.
The problems related to saliva can present as challenging to manage. Drooling and choking on saliva are common issues especially for patients with bulbar onset.
This presentation focuses on the number of approaches to managing this complex problem including natural therapies and pharmacotherapy.
Day 1: Hall C, 4.30 Pm to 5.30 Pm: Palliative Care for Degenerating Neurological Disorders: Psychological IssuesPanickerAnuja SDepartment of Psychiatry, PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India E-mail: anujaspan@yahoo.com
Degenerating Neurological Disorders are characterized by a progressive deterioration of brain function, associated with physical, behavioural, cognitive, and emotional consequences. Patients typically describe high levels of stress, regardless of the extent of their physical disability, secondary to the resulting impairments in personal, familial, social and work functioning. They are also at a higher risk of developing stress-related disorders such as anxiety and depression. The presence of depression and other neuropsychiatric symptoms have a negative impact on the quality-of-life of patients and caregivers, which can be a factor in accelerating cognitive decline. This paper will put outline the psychological issues associated with Degenerating Neurological Disorders and psychological methods for management of the same.
Keywords: Degenerating neurological diseases; psychological issues; palliative care
Day 1: Hall C, 4.30 Pm to 5.30 Pm: Palliative Care in Degenerating Neurological Disorders: Handling Practical Nursing Problems: Palliative Care Nursing Challenges in Patient with Motor Neurone DiseaseMuraliShakilaDepartment of Palliative Medicine, Christian Medical College, Vellore, Tamil Nadu, India E-mail: shakila.m@rediffmail.com
Motor Neurone disease is a progressive disorder that can result in significant disability and functional impairment. This sometimes equates with belief that there is”nothing more to be done”. This feeling of hopelessness and despair is frequently sensed by patient and families.
Symptoms due to upper motor neuron, lower motor neuron or bulbar pathology may lead to, dysphagia, spasticity, respiratory distress and emotional lability etc, thus impairing activities of daily living and safety.
This presentation will focus on cost effective methods of evidence based nursing care of patients with progressive degenerative motor neuron disorder. Constructive and co-ordinated fashion of multidisciplinary team will help the patient to receive better quality of care, and increase the confidence of caregiver.
Keywords: Degenerative neurological diseases; palliative nursing; motor neuron disease
Day 2, Hall A: 8 Am to 9 Am: Film Viewing: “The Choice Is Yours”AndersonKarenSchool of Arts and Humanities, Edith Cowan University, Perth, Western Australia, Australia E-mail: karen.anderson@ecu.edu.au
This is a documentary film on the life and philosophy of one of the world's great psychiatrists, Dr Victor Frankl, with a focus on cancer and palliative care.
This inspirational 45 minute documentary film was written, directed and produced by New York filmmaker, Ruth Yorkin Drazen for the American Board of Internal Medicine Foundation (ABIM). Frankl's philosophy inspires self-reflection as one searches for the meaning of life. His theories are being taught and utilised worldwide.
Transforming reflections from patients with cancer, multiple sclerosis, and degenerative brain disorder are incorporated into the film along with those of three physicians who are cancer survivors – Edwin Cassem, MD, Professor of Psychiatry, Harvard Medical School, plus Bruce Chabner, MD, Clinical Director of MGH Cancer Centre and Chief of Haematology/Oncology, Massachusetts General Hospital, Boston, plus Balfour Mount, MD, Eric Flinders Chair, Palliative Care Medicine, McGill University, Montreal, Canada.
‘The Choice is Yours’ won the 2003 International Health and Medical Media Award and also received the Patient Care Award and the Surgeon Generals Award in the same year. This film will be of interest to everyone – doctors and physicians, medical and health professionals of all disciplines, cancer patients and survivors together with their family members and friends, volunteers and others interested in the search for meaning.
The primary goals the film achieves include the enhancement of one's sense of being and the meaning of life; the promotion of self-reflection as a healthy habit of competence; improvement of the doctor-patient relationship within the context of communication, humanism, empathy and love of mankind; and the reaffirmation of the value of patient dignity.
After viewing the film: Take time to discuss and consider your responses. The following questions may be useful:
How, if at all, has viewing this film impacted upon you?
What gives meaning to your life?
In what ways might viewing this film impact upon how you live your life now and how you do the work you do?
Suggested reading of books by Dr Victor Frankl:
Frankl, V.E. (1977). Man's Search for Meaning: An introduction to logotherapy (8th ed.). London: Hodder and Stoughton
Fabry, Joseph & Fabry, Judith (Trans.). (2000). Recollections Victor Frankl: An Autobiography. Cambridge: Perseus Publishing
Klingberg, H. (2001). When Life Calls Out to Us: The Love and Lifework of Victor and Elly Frankl. New York: Image
Keywords: Doctor-patient relationship; logotherapy, life philosophy
Day 2: Hall A, 11 Am to 12 Pm: Hidden Lives Hidden Patients: In Patients with Severe and Persistent Mental Illness. Palliative Care for Severe Persistent Mental Illness: An Approach Whose Time Has Not Yet Come for Developing Countries?TrachselManuel12HodelMartina A1Institute of Biomedical Ethics and Medical History, University of Zurich, Zurich, SwitzerlandDepartment of Psychiatry, Cedars-Sinai Health System, Los Angeles, USA E-mail: manuel.trachsel@gmail.com
Background: As a significant number of terminally ill patients receiving palliative care suffer from states that include anxiety, depression, or delirium, healthcare professionals from psychiatry and palliative care collaborate to provide an integrated approach. However, despite this well-established collaboration, psychiatry does not currently or explicitly provide palliative care for patients with mental illness outside the context of terminal medical illness. We argue that patients with severe persistent mental illness (SPMI) would benefit from a palliative approach, with a focus on symptom control and other psychosocial factors that might serve to enhance their quality of life.
Discussion: Based on the WHO definition of palliative care, we propose a definition of palliative psychiatry, in which the beneficiaries are patients with SPMI who are at risk of therapeutic neglect or overly aggressive care within conventional paradigms. These include patient groups who experience high degrees of suffering, such as long-term residential care patients with severe chronic schizophrenia or therapy-refractory depression patients with persistent suicidal ideation. We will discuss clinical and ethical considerations, with particular regard to whether palliative psychiatry is equally meaningful in a developing country where resources for and access to standard interventions may still be limited.
Conclusion: For patients with SPMI who fail to benefit from standard treatments, a palliative care approach can potentially improve quality of care, person-centredness, and patient autonomy. Palliative care does not mean giving up on the patient but rather involves redefining the goals of care and accepting the reality that mental illness can be fatal.
Keywords: Autonomy, palliative care, psychiatry, quality of life, severe persistent mental illness
Day 2: Hall A, 11 Am to 12 Pm: Hidden Lives Hidden Patients: In Transgenders: LGBT: Shalom Delhi -Caring for Transgenders Living with HIVDuomaiSavitaShalom Delhi and Palliative Care Service, Emmanuel Hospital Association, New Delhi, India E-mail: savita.duomai@eha-health.org
Delhi has a significant number of transgenders in the city, with a high prevalence of HIV infection among them. HIV adds an additional layer of stigma to their already marginalized existence. Access to quality health services remains a challenge, and many whose resources are meager are pushed further into poverty by their illness. Testing for HIV is often at a late stage when the illness has already advanced and taken its toll. Depression, anxiety and addictions are common as also poor adherence to anti-retroviral medication. Livelihood is adversely affected because of poor health and recurrent infections. Stigma that is often internalized, significantly adds to the emotional and mental trauma experienced by them.
Shalom Delhi, A Palliative Care Unit of Emmanuel Hospital Association, has been caring for transgenders with HIV since 2009. A trusting relationship has developed over the years contributing to increased acceptance of Shalom's services by transgenders. In-patient and out-patient medical services for treatment of opportunistic infections are provided at the health center at a highly subsidized cost. Staff regularly visit the homes of transgenders to provide long term supportive care. Counseling on initiation and adherence of antiretroviral medicines, health education, self-care and prevention of transmission is given both at the hospital and during home visits. Support groups of transgenders have been formed and regular meetings are held to discuss issues relevant to them. A pilot livelihood program was started to provide livelihood support, and Shalom hopes to expand this in the future.
Keywords: HIV/AIDS; mental health issues; transgender
Day 2: Hall B, 10 Am to 10.45 Am: Palliative Care and Noncommunicable Diseases: Healthy India Alliance: Prioritising Palliative Care in Noncommunicable Disease Prevention and ControlKathuriaPrachiHRIDAY, New Delhi, India E-mail: prachi@hriday-shan.org
The Healthy India Alliance- for the prevention and control of NCDs [HIA], established in October 2015, is a coalition of multi-sectoral Civil Society Organisations (CSOs) to address Non Communicable Diseases (NCDs) by generating awareness, building capacity, empowering CSOs, patients and advocating for health promoting norms and policies. HIA's vision is to catalyse multi-sectoral action to enhance health and quality of life in India (www.healthyindiaalliance.org). The mission is to create an enabling environment for active participation of health and non-health CSOs to prevent and control NCDs through effective policies, programmes and partnerships. Established under the aegis of the NCD Alliance (www.ncdalliance.org), HRIDAY houses the Secretariat of the HIA.
In 2013, India adopted a set of ten national targets under the National Action Plan to reduce premature NCD mortality by 25% by 2025, following the World Health Organizations’ Global Action Plan for the Prevention and Control of NCDs, 2013-2020. The National multi-sectoral Action Plan for the Prevention and Control of NCDs developed by the Ministry of Health and Family Welfare, Government of India (MoHFW, GoI), calls for multi-sectoral engagement and coordination to achieve these targets. Civil Society Organisations have been identified as an important partner in the Action Plan to achieve the National NCD targets. Palliative care is an essential component of a comprehensive response to NCDs, as outlined in the WHO global action plan for the prevention and control of NCDs 2013–2020. In 2015, just over 50% of countries have included palliative care in their national NCD policy, and nearly two thirds reported some government funding for palliative care.
The MoHFW, Government of India's National Action Plan and Monitoring Framework for Prevention and Control of Non Communicable Diseases (NCDs) in India clearly states that developing and implementing a palliative care policy using cost effective modalities and ensure accessibility to affordable palliative care services is one of the key activity to achieve the target of an 80% availability of essential NCD medicines and basic technologies to treat major NCDs in both public and private facilities.
HIA accords high priority to enhancing civil society engagement (both health and non-health sectors) to highlight the importance of palliative care in NCD prevention and control. The Alliance calls out for all community members to join in the movement for reducing exposure to NCD risk factors at an early age, as well as prioritizing issues of people living with NCDs. The Alliance fosters to empower peopliving with NCDs as advocates to participate in advocacy efforts at with policy makers and grassroot level communities. The Alliance is committed to make efforts towards understanding the needs and expectations of patients living with NCDs, their rights and responsibilities and identifying/developing platforms to engage them as advocates. The Alliance provides a platform for synergistic action between palliative care professional and CSOs working on NCD related issues to decode the relevance of engaging patients in NCD prevention and control at different levels: individual, societal, state and national levels.
The Alliance works in partnership with MoHFW, GoI and the World Health Organization. They have acknowledged the potential of HIA to have a positive impact on CSO engagement for the prevention and control of NCDs.
Keywords: Non communicable disease; palliative care; WHO
Day 2: Hall B, 10 Am to 10.45 Am: Palliative Care and Noncommunicable Diseases: Scope for Palliative Care through Noncommunicable Disease Programs in IndiaVallathNandiniTrivandrum Institute of Palliative Care Sciences, Pallium India, Thiruvananthapuram, Kerala, India E-mail: aanandini@gmail.com
Background: Currently, India ranks 130 among 188 countries in human development index which considers life expectancy and per capita income (http://timesofindia.indiatimes.com/india/India-up-5-spots-ranks-130th-in-Human-Development-Index-UNDP/articleshow/50170343.cms) and its position in the latest study on quality of death index done in 80 countries is 67th. The epidemiologic transition is also glaringly apparent with non-communicable diseases (NCD) increasing by two fold or more in 2015 in comparison with that in 2005. Reflection of this is seen again when we look into the causes of deaths in India. If 52.8% of deaths were due to NCD in 2005, it increased to 59% in less than ten years in 2015. More than forty millions of Indians are driven to poverty due to out of pocket expenditure alone due to the escalating cost healthcare. Palliative care which is firmly centred on the quality of life of person with life-limiting diseases and appropriate timely care, does not reach even 2% of those who need it. India has 415 palliative care centers for 1.3 billion citizens.
Initiatives from the Central Government: Within this background, the formulation and submission of national palliative care strategy in 2012 to the Ministry of Health was a milestone achievement by the pioneers in the field. This transitioned into National Program for Palliative Care [NPPC] and sought budget as the 12th five-year plan, but failed and the implementation of this program at state levels, was delayed until 2014 due to lack of funds. In 2014, some budget allocation was achieved through the National Health Mission. Palliative care program is now merged within the existing National Program for Cancer, Diabetes, Cardiovascular disease and Stroke (NPCDCS) and National Program for Health Care of Elderly (NPHCE). Ten percent share of the budget meant for National Program for Cancer is available for developing palliative care facilities in tertiary hospitals and for medical college hospitals with cancer care facility. Unfortunately, the purpose is open to interpretation. This means, this budget may be used for financing a radiotherapy machine – if shown as being used for palliative radiation. The NHM Flexipool budget for NCDs support palliative care service development at district and sub-district levels. The budget supports the salary of the state level program co-coordinator and data entry operator and infrastructural needs of the state palliative care cell. At district level, Rs.48,40,000 is available for districts for infrastructural support, developing outpatient and inpatient facilities with ten beds. The salary of a physician, 3 nurses and data entry personnel is supported at district hospital level. Community Health Centers are expected to run biweekly outpatient clinics and primary health centers are to expected to identify and refer patients with palliative care needs and work on creating awareness about the field amongst the public using the existing staff in the NCD program. All states are expected to submit the Program implementation plan [PIP] through the section B27 of the NCD PIP to receive 60% of the projected expenses from the center. The proportion for the north-east and hilly states is higher with the centre supporting with 90% of the share. NHM-NCD framework for palliative care has the advantage of integrating palliative care within the existing health delivery system. The openness in the framework to associate with the experienced NGOs in the field for training would help with the much needed capacity building. The insistence on minimum six weeks training as criteria for the newly created government posts assures some quality of services. There are major deficiencies. For example, there is no palliative care cell at the national level. The governance and monitoring structures are undefined.
Initiatives from the State Government: Kerala declared its state policy in 2008 and has about 315 palliative care centers of which 167 are Recognized Medical Institutions [RMIs]. The services are available mostly around NGO sector and through public healthcare framework at district and lower levels. Besides patients with cancer, those with diabetes, mental ill-health and neurological disability are included within the folds of palliative care. Palliative care has not made entry into most of the tertiary care hospitals nor into medical college hospitals. Maharashtra is the second state to frame a policy in 2011 and now has a state palliative care cell with officer in charge and about ten palliative care centers. Recently in 2016, Karnataka has launched it's palliative care policy.
Other Initiatives: National Cancer Grid, a network of nearly 90 cancer care centres in the country, is strategizing and facilitating palliative care into it's recommended best practice through collaborative academics, services and research. Association of Physicians of India is active in associating with the field with blended discussions during conferences and workshops on pain relief across the country. The Indian association of Paediatrics and Indian association of Paediatric Oncology have incorporated the dimension of palliative care and have developed a special interest group or a charter.
Conclusion: As the critical number of stakeholders at policy making levels become aware, our emphasis should continue to focus on normalizing and necessitating palliative care within the healthcare dynamics as good and appropriate medical practice and as minimum mandatory care. It would indeed be unfortunate if this opportunity metamorphosizes the field into another speciality with super-specialist palliative care physicians amongst a new set of techno jazz.
Keywords: Community health centres; non communicable diseases; palliative care; India
Day 2: Hall C, 10 Am to 10.45 Am: Opioids - Updates: Pain Management in People with Opioid DependenceAmbekarAtulNational Drug Dependence Treatment Centre, AIIMS, New Delhi, India E-mail: atul.ambekar@gmail.com
Opioids are among the best analgesics known in the medicine. Opioids are also one of the best euphoriants and intoxicants known to the mankind. It is not surprising that almost all the opioids possess significant abuse and dependence liability. However very few patients who receive opioid analgesics for the management of chronic cancer pain develop ‘opioid use disorders’ (i.e. addiction or ‘dependence’ as understood in behavioral sciences). Nonetheless, identification and management of opioid use disorders in this subgroup of patients remains challenging.
Major challenge however, is the inadequate availability of opioid for the management of pain or for the management of opioid addiction, globally, but more so in India. A sizable proportion of people who use opioid drugs in India, use opioid pharmaceuticals. Yet, the regulatory framework of India, while restricting the opioid pharmaceutical availability for the legitimate patients, has not been able to effectively control the diversion and misuse of opioids. There is an urgent need to bring about legal and policy reforms to ensure that illicit use of opioids is effectively controlled and yet, opioid medications are accessible to those patients who need them for the management of chronic pain or for opioid addiction.
Day 2: Hall A, 12 Pm to 1 Pm: Hidden Lives Hidden Patients: In Natural Calamities (Earthquakes): Natural Disasters - Relevance of Palliative CareMundayDanielPalliative Medicine and Health Services Research, International Nepal Fellowship, Kathmandu, Nepal E-mail: d.f.munday@googlemail.com
The needs of vulnerable people (with advanced chronic illness, frail elderly and people with severe disability) who are affected by natural disasters and who possibly require palliative care have not often been considered. However, following Hurricane Katrina in New Orleans in 2005 where 71% of the 1836 who died were over 65, researchers and service providers began considering the needs of this vulnerable group.
Natural disasters can have an impact palliative care in several different ways. There could be disruption to existing palliative care services. Institutions such as hospices might find it difficult to relocate patients to places of safety. The experience in the immediate aftermath of Hurricane Katrina was that facilities such as nursing homes were particularly severely affected and because of lack of planning they did not have robust policies in place to ensure that their residents were safe, leading to deaths which could have been avoided. People who are severely injured and who will die of their injuries either following treatment, or because medical services are not able to cope need to receive urgent palliative care to control their symptoms and provide relief of their suffering. With normal services either non-functional or overwhelmed following the disaster, delivering palliative care to those affected will fall to emergency relief teams who are trained and equipped to deal with injuries and acute illnesses, such as epidemics occurring as a result of the event, rather than to deliver palliative care.
As more people in low and middle-income countries (LMIC) suffer from advanced non-communicable disease and global warming leads to an increase in incidence and seriousness of natural disasters, these issues affecting palliative care will become increasingly important globally. LMIC frequently have services which struggle to operate even in optimal conditions and therefore are more unlikely to withstand the damaging effects of natural disasters.
A recent scoping literature review of literature investigating palliative care needs of people affected by natural disasters in LMIC revealed no studies particularly focusing on palliative care. However, some studies did focus on older people and those with non-communicable diseases. Epidemiological studies reported that vulnerable people were more likely to die in disasters. Some papers revealed that post-traumatic stress was common in older people following natural disasters, although there was some evidence that older people were particularly resilient and were no more likely to suffer psychologically than younger individual. Several studies reported that whilst chronic disease management is a common health care need encountered by rescue teams in post-disaster situations, they were normally poorly equipped to provide it.
This presentation will explore the issues regarding palliative care following natural disasters and will draw on work we are currently undertaking in Nepal following the April 2015 massive earthquake.
Day 2: Hall A, 12 Pm to 1 Pm: Hidden Lives Hidden Patients: Elderly Neglect Care: Elder Neglect and Abuse: The Relevance of Palliative CareGaneshAlkaDepartment of Geriatrics, GKNM Hospital, Coimbatore, Tamil Nadu, India E-mail: alkaganesh8@gmail.com
The needs of the elderly now occupy an important focus for health care professionals, social scientists, economists and political scientists, because of increasing numbers of elderly, who have declining well being. The negative impact of disease, disability, shrinking incomes, changing societal norms, and loss of vocation, have cumulatively resulted in dependency, poverty, loss of dignity and marginalization of the elderly. These factors prompted the international community through the United Nations to enunciate a policy statement in 1991 regarding the rights of the elderly. These are outlined as, the right to independence, participation, care, fulfilment, and dignity.[1] However, these rights remain mainly on paper due to multiple factors, including that of elder abuse and neglect.
Elder abuse is defined a “single or repeated act, or lack of appropriate action, occurring within a trusting relationship, causing distress or harm to a vulnerable older person”. The various types of abuse and neglect have been categorized as physical, emotional and psychological, financial, and sexual. Family members, and paid carers within the home or in institutions are responsible for most forms of abuse. The problem is difficult to detect because health care professionals are not trained to detect it. The victim of abuse is often unable to report abuse. A WHO study in India showed that senior citizens, though admitting that maltreatment and psychological distress does occur, were reluctant to label these behaviours as “abuse”. The participants, in fact, seemed to justify neglect, blaming changing value systems.[2]
Caregiver stress, and frustration, especially when dealing with frail, highly dependent cognitively impaired persons is a common scenario of abuse. Training of health professionals to detect such situations is a first step. Thereafter, improving patients autonomy, and reducing caregiver burden can be helpful. Relief of symptoms such as pain, dyspnoea, and reassuring carers that professional support is available can be helpful.[34]
Clearly research is needed to find reasons why such behaviour occurs, how detection can be facilitated, and how to introduce preventive measures.
R<sc>EFERENCES</sc>UN General Assembly, Resolution No. 46/911991SonejaSElder abuse in India. WHOLast accessed on 2016 Dec 30Available from: http://www.who.int/ageing/project/elder_abuseJayawardenaKMLiaoSElder abuse at end of lifeJ Palliat Med2006912736HarrisDForget me not: palliative care for people with dementiaPostgrad Med J2007833626Day 3: Hall A, 11 Am to 11.45 Am: Recent Palliative Care Developments in India – Eastern India: Integration of Palliative Care into the Healthcare System – East Zone ReportBoraSanghamitraDepartment of Palliative Oncology, North East Cancer Hospital and Research, Guwahati, Assam, India E-mail: sanghamitrabk@gmail.com
Background: India has seen several improvements in the recent years in its palliative care scenario including the creation of a National Program for Palliative Care (NPPC) by the government of India in 2012. The year 2014 saw the landmark action by the Indian Parliament, which amended India's infamous Narcotic Drugs and Psychotropic Substances Act, thus overcoming many of the legal barriers to opioid access. Several recommendations have been made in recent years for implementation of National Policy, opioid availability, education and capacity building. There have been petite but significant developments in individual states in this regard. This study describes the present status of palliative care in the eastern states of Bihar, Jharkhand, Odisha, Sikkim, Chattisgarh and West Bengal.
Objectives: The objectives are: (1) To evaluate the extent of integration of palliative care into the healthcare system in the eastern states of Bihar, West Bengal, Sikkim, Chattisgarh, Odisha and Jharkhand. (2) Enumerate and describe supportive policy from the state governments. (3) Existing process of programme and the need for policy implementation. (4) Relationship of the integrated model with NGOs/Civil Society Organisations. (5) Highlight future plans/goals?
Result: It is worthwhile to say that there have been palpable developments in these states with Odisha having the fastest change. The State Government has planned to establish pain and palliative care centres at 5 district headquarters hospitals (DHHs). The state of Jharkhand is now planning for a state palliative care policy. Bihar, Sikkim, Chattisgarh and West Bengal are still to have some integration of palliative care.
Conclusion: It can be concluded that there can be successful implementation of palliative care programs if there is a collaborative effort of the state machinery and palliative care working groups/NGOs/agencies as stakeholders. It is important to explore the gaps in collaboration and policy implementation.
Day 3: Hall B, 11 Am to 11.45 Am: Nurturing Relationships: Doctor Patient Relationship in Indian ContextKCRajashreeDepartment of Palliative Care, Malappuram Initiative in Palliative Care, Malappuram, Kerala, India E-mail: drrajisuresh@gmail.com
The word patient came from the Latin word ‘Patiens’ which means sufferance. Hence the purpose of medical practice is anchored on relieving suffering! Communication with the patient, in a medical encounter, is immensely skilled.
The basic principle while communicating with the patients is to listen to their narration and clarify wherever required. A doctor needs to spend sufficient time with the patient to understand the condition and concerns correctly. The doctors in Indian settings are overloaded with work which invariably squeezes time available to listen to their patients. Relieving the clinicians from administrative responsibilities can help the situation to an extent.
Extending patient centred care to family centred and community centred care can improve doctor patient relationship. This will help in healthy outcome in large number of people. In India, generally, information about the illness is shared among the family members irrespective of the patient's wish. Family plays a significant role in health care and often a responsible family member will be the decision maker!
The media plays a major role in facilitating the doctor patient relationship by giving the correct information at the right time in an appropriate manner. On the other hand, wrong messages given by the media can impart a negative image of the health care system and health professionals.
Another important point is to strengthen the medical education by inclusion of topics like Principles of communication, Ethics, Standards and legal aspects of medical practice, Health literacy, Patient education and empowerment, Audit, Grievance redressal mechanisms and Operational research. Out of these, effective communication and ethical practice are of utmost importance and become vital in end of life situations.
Interpersonal communication skills are considered to be core competencies for Palliative Care. Professionals in India encounter challenges for effective communication due to inadequate training, socio cultural diversity and organisational issues.
Keywords: Communication; cultural diversity; doctor-patient relationship
Day 3: Hall B, 11 Am to 11.45 Am: Nurturing Relationships: Life after LossKrishnaswamyManjulaJeevodaya Hospice, Chennai, Tamil Nadu, India E-mail: manjula6693@yahoo.co.in
Loss is when something or someone is taken away from a person. It is permanent; it is irretrievable or irreplaceable; and more often than not it is unexpected. These three components form the essence of loss in palliative care.
We have to deal with two types of loss, one that affects an individual and the other that affects someone very close to the individual. In both cases, the loss is permanent, life changing, life threatening and which has every likelihood of culminating in death. In the case of an individual, the losses are many but the loss of self esteem is most hurting and family, friends and professional carers have each a role to play in restoring the person's self confidence to continue with life. In the case of a person having to deal with the suffering and impending death of someone close, equal care is warranted to ensure that they are able to live through the painful experience of impending death by acknowledging anticipatory grief. Once death occurs, time must be allowed for normal grief. However signs of prolonged or complicated grief must be anticipated in the vulnerable group and appropriate professional help must be sought. Grief in children, does not just depend on the chronological age, other factors such as maturity, family and social circumstances also play a part. The family and professional carers must have awareness and skills to deal with individual cases.
Keywords: Caregivers; complicated grief; grief and bereavement
Day 3: Hall C, 11 Am to 11.45 Am: Rehabilitation and Palliative Care – Being a User and ProviderMPAshla RaniPallium India, Trivandrum, Kerala, India E-mail: ashla@palliumindia.org
Traditional palliative care as it evolved in the West does not seem to be inclusive of people with paraplegia and quadriplegia. Understandably, it does not have to in the West, because there is a parallel stream of rehabilitation medicine that takes care of it. But in low and middle income countries as in India, people with life-limiting paralysis are given high-tech aggressive treatment in the beginning and then they are sent home with no support system at all. Changing a urinary catheter every three weeks involves unbelievable torture of travel and financial loss. In no time at all, pressure ulcers develop and eat their way into the body. Contractures set in preventing any further rehabilitation.
Those who created the palliative care system in Kerala were compassionate enough to consider that the definition of “life-threatening” could be inclusive of lives threatened by four walls, by pressure ulcers, contractures or huge psychosocial issues.
I had an accident six years ago. I cannot use my legs and most of my arms. I was a patient, and only a patient, for 4 years. Today, I continue to be a patient for about an hour a day when someone help me with my daily activities. For the rest of the time, I am part of a team of palliative care providers. I work a full day, as the chairman's executive assistant, as a friend helping other people with paralysis in our half-way-home and as a friend to children of bereaved families.
Palliative care can give quality, purpose and meaning to lives like mine so that we can not only receive, but also give.
Keywords: Palliative care; paraplegia; India
Day 3: Hall A, 11.45 Am to 12.15 Am: Mindfulness in Chronic DiseasesSharmaMahendra PDepartment of Clinical Psychology, National Institute of Mental Health and Neuro Sciences, Bengaluru, Karnataka, India E-mail: sharma.mahendra81@gmail.com
Many philosophical, spiritual, and psychological schools and approaches give emphasis to the significance of the prominence of consciousness for the protection and enrichment of well-being. In spite of this, it is easy to oversee the significance and role of consciousness in the prevention and promotion of well-being as attention and awareness are its primary dimensions. The mindfulness is one attribute of consciousness that has been discussed extensively in relation to well-being. Meditation is one of the most significant contributions made by India to the world civilization. Vipassana Meditation, which is also known as Mindfulness Meditation is one of the meditative techniques developed in ancient India. Mindfulness involves intentionally bringing one's attention to the internal and external experiences occurring in the present moment, and is often taught through a variety of meditation exercises. This relaxed non-bias awareness allows one to see things clearly as they really are and learn to respond, rather than react to stressors encountered. In the current empirical literature, clinical interventions based on training in mindfulness skills are described with increasing frequency, and their popularity appears to be growing rapidly.
Research on mindfulness has indicated overall positive effects and improvement in stress, spirituality, inter-personal relationship, self-care practices, well-being and enhance compassion and presence in patients and other non-clinical populations. However, very limited number of studies has been conducted on terminally ill patients and their professional caregivers using mindfulness-based interventions. The Present talk will provide theoretical and conceptual understanding of mindfulness and its application in palliative care setting with a brief demonstration of mindfulness meditation.
Keywords: Mindfulness; meditation; palliative care
Day 3: Hall B, 11.45 Am to 12.15 Am: Interventional Therapies in the Continuum of Care: Interventional Therapies in Cancer PainBhagatSurbhiDepartment of Pain Medicine, VNCC, GKNM Hospital, Coimbatore, Tamil Nadu, India E-mail: surbhipbhagat@hotmail.com
Interventional pain control is an alternative approach to pain relief. It is required in only small number (8-11%) of cancer patients who are not amenable to systemic analgesia, either because of intolerable side effects or pain that is refractory to treatment.
These patients are referred to specialist pain clinics either by request of oncologist or treating palliative care physician. Most often than not it reflects the desperation on the part of the referring physicians, patients or their relatives. However after carefully considering the risk vs benefit, such procedures must be offered.
Options range from procedures interrupting the somatic, visceral or central neural pathways via destructive or non destructive techniques.
Although the evidence is less, skills and knowledge in this field is rapidly developing and the use of interventional techniques have proved to be important and successful part in multimodal pain control in cancer patients, despite the prognosis of these patients being limited.
ORAL FREE COMMUNICATIONS: Oral-01: Implementation of a Standardized 6 Weeks Residential Palliative Care Course for Doctors and Nurses in India-Preliminary 2 Year Results and OutcomesReddySureshVallathNandini1GuptaMona2GujelaManoj1NaikNavami1MohanSarath3MRRajagopal3MD Anderson Cancer Center, Houston, Texas, USDepartment of Palliative Care, Indo-American Cancer Association, Texas, USCase Western Reserve, Cleveland, USATrivandrum Institute of Palliative Care Services, Pallium India, Thiruvananthapuram, Kerala, India E-mail: sreddy@mdanderson.org
Background: The Indo-American Cancer Association (IACA), and Trivandrum Institute of Palliative Care Sciences (TIPS), India, have jointly developed a six week residential course in PC with a standardized curriculum for physicians and nurses across pre-selected centers in India.
Objectives: To administer a standardized Pallium Care (PC) curriculum through a six weeks of residential course at preselected centers in India, and measure the knowledge domains before and after the course, including participant satisfaction and the long term outcome of the course.
Methods: A core team of PC experts from India and US developed a comprehensive six week course. The curriculum was administered at five institutions, selected on the basis of mandatory criteria, and included both nurses and physicians. The delivery of the course was through a standardized schedules, covering a pre-set curriculum, combining class room didactics with clinical rotations in different settings. Feedback data was mandated and collected at predetermined intervals throughout the course. A long term impact questionnaire was administered at 6, 12, and 18 months.
Results: A total of 53 candidates completed the course with 27 (51%) physicians and 26 (49%) nurses in five centers. In the pre and post survey of knowledge domain, there was a significant improvement in all the domains. There was a high level of satisfaction in the training standards, faculty involvement, and overall satisfaction of the course.
Conclusion: The IACA-TIPS initiative has created a comprehensive curriculum through its collaborative process of content development. Mandatory standards were used for selection of centers to safeguard adequacy in terms of staff and clinical setting. Evaluation methods used at predetermined intervals helped to maintain high standards and implement changes throughout the course. The experience and the results may be utilized to recruit new centers, thereby increasing PC workforce among physicians and nurses in India.
Keywords: Curriculum evaluation; India; palliative care
Oral-02: Assessment of Knowledge, Attitude and Practice of Oncologists Regarding End of Life Care: Survey in a Tertiary Cancer CentrePatraLipikaKarunashraya, Bangalore Hospice Trust, Bengaluru, Karnataka, India E-mail: drlipika.patra@gmail.com
Introduction: Advanced stage cancer patients present a major challenge to physicians because of their huge burden of physical and nonphysical symptoms. When the benefit of anti-tumour therapies is outweighed by either the risk or burden of treatments, it is the oncologist who must direct the patients and the family to initiate a care plan that focuses on symptom palliation and other efforts to reduce suffering, maintain quality of life, and prepare for the end of life. The physician's clinical competence, willingness to participate in the process and empathetic reassurance are essential in helping patients and families in their last hours.
Methods: A cross-sectional survey was conducted among 30 oncologists using a self-administered questionnaire. The questionnaire was developed from the course module formulated for EOLC Certificate Program by Indian society for Critical Care Medicine (ISCCM) and the Indian Association of Palliative Care (IAPC). The dependent variables included knowledge, attitudes and practice of end-of-life care in their hospital.
Results: Only 30% of oncologists considered themselves to be confident to deal with EOLC issues. The majority were medical oncologists. All of them felt that lack of knowledge was the barrier in communicating EOLC related decisions. Conversely, almost half of surgical and radiation oncologists felt lack of time to be the main issue. About 40% of the oncologists felt that barriers to effective EOLC at their hospital were legal issues and fear of litigation. Over 60% agreed that they should be part of bereavement care.
Conclusion: The findings emphasize the need for initiatives to improve the basic knowledge regarding EOLC, preferably through CMEs or workshops. It is important to develop strategies to minimize the risk of burnout and to educate Oncologists about legal issues involved.
Keywords: Attitude, bereavement care, clinical competence, knowledge, practice
Oral-03: An Evaluation of Nurse Prescribing in Palliative Care in Uganda: A Mixed Methods StudyJuliaDowning12WilsonAcuda3DorothyAdong3EmmanuelLuyirika4FatiaKiyange4RKiwanuka5JAmandua6LizGrant2MLeng127The Evaluation Research TeamMakerere and Mulago Palliative Care Unit, Makerere University, Kampala, UgandaGlobal Health Academy, University of Edinburgh, EdinburghHospice Africa Uganda, Kampala, UgandaAfrican Palliative Care Association, Kampala, UgandaPalliative Care Association of Uganda, Kampala, UgandaMinistry of Health, Kampala, UgandaCairdeas International Palliative Care Trust, Scotland E-mail: julia.downing792@btinternet.com
Background: Specially trained palliative care (PC) trained nurses in Uganda have been able to prescribe since the change in the legislative statute in 2004, thus increasing access to PC. This is of global interest but needed full evaluation to determine the effectiveness of the nurses role; in particular prescription of oral morphine and assess the transferability to other countries.
Methodology: 3 part evaluation (1) Preparation of the nurses for the role (2) Process of assessing and managing the patient’s’ pain, including the prescription of oral morphine and patient outcomes; (3) Appraisal of the health system and context. Mixed approach undertaken including: curriculum review; semi-structured interviews, use of the APCA POS; chart and prescription review, rapid systems appraisal (RSA) methodology. Ethical approval was obtained. 17 nurses, 4 trainers and Ministry of Health participated in curriculum interviews; 22 nurses each recruiting between 10 and 20 patients participated in prescribing and outcomes data collection over 3 clinical contacts and 10 districts assessed using RSA and the military hospital.
Results: Results show that the nurses are able to assess and manage pain, including the prescription of oral morphine though some minor curriculum adaptations are recommended. Themes identified; improvements to training, supervision and mentorship, competency, boundaries of practice, beliefs and system issues. Prescribing and outcomes data analysis demonstrates ability to assess and manage pain, give appropriate medications and reassess. RSA showed variability in access to medications with regular stock-outs, limited understanding of PC and opiophobia. It also showed resilience and determination in nurses to overcome challenges and improve access to PC.
Conclusion: Whilst challenges exist and recommendations will be made to improve the system, this evaluation has clearly shown the benefit and safety of nurse prescribing of oral morphine for PC in Uganda, and recommends the extension of nurse prescribing to other countries.
Keywords: Evaluation, nurse prescribing, palliative care
Oral-04: Noncommunicable Diseases and Palliative Care Needs: A Survey of a Rural Hospital in NepalBKManjuMundayDanielPowysRuthInternational Nepal Fellowship, Kathmandu, Nepal E-mail: daniel.munday@inf.org
Background: In low-income countries increasing numbers of people are suffering from non-communicable diseases (NCD). Clinical experience backed up by admission statistics from a 166-bedded hospital in rural West Nepal indicated that increasing numbers of patients with COPD, cardiovascular disease, alcoholic liver disease (EtOHLD) and cancer were presenting to the hospital. We undertook a survey of patients admitted with NCD and palliative care needs to inform service development at the hospital.
Method: Cross-sectional survey of inpatients (all wards apart from obstetric) was conducted over five days. Patients with NCD were identified and those with palliative care needs (PCN) were identified using an indicator tool SPICT™. Patients’ symptoms were recorded using a standardized questionnaire.
Findings: 234 inpatients were identified, 66/234 (28%) with NCD. 52/61 (85%) on the medical ward had at least one NCD. 23/66 (35%) patients with NCD were identified as having PCN. 18/66 (27%) had COPD, 13/18 (72%) with PCN. CVA (4, 1PCN), renal disease (4, 1PCN) Diabetes (4), heart failure (3, 2PCN) myocardial infarction (3), and rheumatic heart disease (3, 1PCN). Two patients had cancer (both advanced stage) and two had end stage EtOHD (all four with PCN). 19/23 patients were interviewed for symptom burden (others too unwell or died before interview). 19/19 (100%) complained of pain, shortness of breath, weakness and tiredness; 16/19 (84%) dry mouth, 10/19 (53%) poor appetite, 8/19 (42%) cough, 8/19 (42%) nausea and vomiting, 3/19 (16%) constipation, 3/19 (21%) cachexia and 2/19 (11%) delirium.
Conclusion: Large numbers of patients with NCD were admitted to this rural hospital, over 1/3 of whom had palliative care needs. There is no oncology facility here and fewer cancer patients are admitted; therefore palliative care should largely focus on non-cancer NCDs. No children were identified. This study, although limited by its short duration, found proportions of NCDs corresponding with hospital statistics.
Keywords: Needs assessment, noncommunicable disease, palliative care
Oral-05: Development of Palliative Care Services in Nepal: An Oral History ProjectBasnyatReginaMundayDanielPowysRuthPaudelBishnu1WinslowMichelle2International Nepal Fellowship, NepalNational Academy of Medical Sciences, Kathmandu, NepalSchool of Nursing, University of Sheffield, Sheffield, UK E-mail: daniel.munday@inf.org
Background: Modern palliative care was first established in Nepal in the late 1990s. After steady growth Nepal was classified as achieving “generalized provision” in the Global Atlas of Palliative Care (2013). Oral history is the collection and study of historical information from people who participated in or observed past events. Interviews exploring memories and perceptions are recorded, analysed and preserved as a resource for future generations. This project aims to map development of palliative care in Nepal.
Method: Interviews with leaders in palliative care development were conducted. Participants were identified through the Nepalese Association for Palliative Care (NAPCare). Interviews used a life story approach; topics included personal and professional background, how interest in palliative care had arisen and experiences of developing palliative care at local and national levels. Interviews were audio recorded in English or Nepali and transcribed verbatim. Nepali interviews were translated into English and analysed thematically.
Results: 10 interviews have been completed with individuals involved in early development of Palliative Care. Interest in palliative care is often developed by witnessing the suffering of patients with cancer who frequently present late. For others introduction to palliative care was through an opportunity for training abroad. Services started opportunistically often following persistent advocacy, by colleagues joining forces to establish NGOs or through opportunities arising from international support. Other accounts included the history of morphine licensing and manufacture in Nepal and the development of educational programmes. NAP Care was a relatively late development, with several participants recalling how colleagues had almost simultaneously realized the need for a national organization.
Conclusions: Oral histories have provided unique personal and professional insights into palliative care development in Nepal. Further interviews with others including international colleagues will allow further understanding of enablers and barriers to palliative care development.
Keywords: Education, Nepal, opioids, oral history, palliative care
Oral-06: Community Palliative Care Planning: An Education Programme for Undergraduate Medical StudentsBarnardAlanBoltonNicole1Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South AfricaDepartment of Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa E-mail: abarnard@intermail.co.za
Background: The burden of cancer, HIV/AIDS and solid organ failure with limited resources for oncology and curative therapy make palliative care essential. Junior doctors feel unprepared for palliative care, therefore undergraduate training is required to prepare doctors for community based primary palliative care. A novel teaching session using a framework of analysis to understand and plan community palliative care reveals some interesting approaches and allows deeper engagement. Students are divided into groups to consider the community palliative care of a patient and family using a case vignette under the following headings: Strengths, Opportunities, Challenges, Knowledge and Stakeholders. The input of the groups is discussed and combined to learn about the implementation of palliative care in the community.
Method: An example of one of the learning artefacts generated by the students for the planning of community care for a patient with end stage renal disease is presented as an illustration of the way that this process facilitates comprehensive care.
Results: The example shows that new insights on community palliative care can be reached in the classroom or at the bedside.
Conclusion: The teaching and learning of community palliative care planning is enhanced in this tutorial environment. The creative response of the participants enhances understanding of the palliative care needs of the patient and the family. The students have the opportunity to explore all domains of the care and also the effect that being a health care professional in palliative care affects them.
Keywords: Community based primary palliative care; education; renal disease
Acknowledgment
Prof Vanessa Burch (University of Cape Town and SAFRI), Ms. Ralf Graves (FAIMER, Philadelphia); Prof Brian Rayner and Associate Prof Nicola Wearne (University of Cape Town); Angelique Remley, Siyabonga Ntuli, Avela Jama, Samantha Mhangwane, Obakeng Manda, Diya Appadoo, Aphiwe Meyiwa, Lindokuhle Mdlenyani and Luvo Mbobo (Medical Students, University of Cape Town).
Oral-07: Collaborative Working between a Hospice Delivering a Home Care Service and a Dental College in Rishikesh, North IndiaWardBrendaMehtaRanjeeta1AeranHermanshu1ChaturvediAditiDepartment of Palliative Medicine, Ganga Prem Hospice, UttarakhandSeema Dental College, Rishikesh, Uttarakhand, India E-mail: brendajward21@icloud.com
Background: The role of dentistry in palliative care is recognised as an important contributor to palliative care in India given the high prevalence of head and neck tumours in the population. This work aims to demonstrate both how dentists can be incorporated into the hospice team and the benefits resulting from such collaborative working.
Method: In 2015 training in palliative care was offered by the hospice team to a local dental college in the region. The principal director of the college fully appreciated the relevance of palliative care training for both dental teachers and the college dental interns. Participants were encouraged to attend and 12 such dentists qualified in the Indian Association of Palliative Care ‘Essentials in Basic Palliative Care’ (5 day training). Those inspired by the training were then offered the opportunity to develop their skills. They received practical training on palliative care through the delivery of the domiciliary service by the hospice team.
Results: All those attending the dental college passed the qualification. An MOU was developed between the hospice and the college. As a result: (1) Over a period of one year, 2 dental trainers have joined the hospice team on one day a week to both contribute their dental skills and learn practical skills in palliative home care. (2) Dentists attend the hospice monthly free cancer camps held by the hospice to contribute to the dental care of cancer patients and to learn from the attending surgical oncologist who specializes in head and neck cancer care. (3) These same dentists, with support from the team, have delivered several sensitization PC sessions to both healthcare professionals and schools to ensure awareness raised. (4) Palliative care practitioners value and learn from the dentistry input of the dental team for e.g improving mouth care, awareness of prosthesis. (5) Needy patients are now eligible to receive free treatments from the college. (6) The dentists wish to also contribute to fundraising.
Conclusion: Collaborative working benefits dentists, palliative care practitioners and patients and should be encouraged. Training of 30 more dentists has occurred this year.
Keywords: Dental care; Hospice; integration; palliative care
Oral-08: Palliative Care in Conflict: A Novel Undergraduate Medical Curriculum in GazaLengMhoira EF123ElessiKhamis4JefferisTony1GilletJanet1CooperColin1GrantLiz1NaimFadel N4AlshaihkalilAnwar4Global Health Academy, University of Edinburgh, EdinburghCairdeas International Palliative Care Trust, Aberdeen, UKPalliative Care Unit, Makerere University, Kampala, UgandaFaculty of Medicine, Islamic University of Gaza, Gaza E-mail: dr@mhoira.net
Background: Palliative care (PC) for those with life limiting illness is particularly needed where there is chronic stress, ongoing conflict, poor access to health care, low availability of essential medications and high rates of non-communicable diseases. Gaza reflects these challenges with an ongoing complex humanitarian emergency. 1.8 million people (1.4 m refugees) live under a 10 year blockade that affects all aspects of life including access to healthcare and educational opportunities A newly formed PC steering group includes representation from Ministry of Health, academics, UN, WHO and international partners who agreed curriculum integration as a priority.
Method: PC core competencies for undergraduate medical students, developed, delivered and assessed using a blended learning experiential model within a 4th year clinical curriculum. 6 core domains identified using the PC Curriculum Toolkit derived from international frameworks and 7 core competencies agreed.
Results: Students participated enthusiastically within a well organised curriculum with excellent collaboration from clinical and academic colleagues in Islamic University Gaza. Feedback from students included evidence of learning and attitude change. ‘Patients cope better when we tell them the truth’, ‘There is never nothing we can do’ ‘They tried to teach us how to respect humans and keep their rights and keep them comfortable’ ‘The course added to the clinical practice makes us feel the suffering of patients and how we can help them’. MCQ assessment (20 questions with 5 stems) average score of 88% post training.
Conclusion: An integrated curriculum with agreed core competencies for PC is an essential component of developing competent PC practitioners and changing attitudes. Future needs include developing trainer capacity within Gaza and participating in the overall policy and service planning for PC integration within a newly convened steering group. This curriculum can acts as a model for other settings in Palestine and has wider relevance.
Keywords: Conflict, curriculum, humanitarian, palliative care
Oral-10: Barriers in Family Caregivers’ Participation in Cancer Wound ManagementPatilParikshitNirbhawaneVivek1GhooiRavindra B1Department of Medical Social Work, Pune, Maharashtra, IndiaDepartment of Cipla Palliative Care and Training Centre, Pune, Maharashtra, India E-mail: drviveksn@gmail.com
Background: Many cancer patients have wounds that are purulent or infested and often foul smelling. These need regular cleaning and dressing, which may have to be done more than once daily. Our centre operates on family care, in which one caregiver of the patient is required to stay with the patient. The caregivers help the staff in managing the patient, but usually shirk the responsibility of dressing the wounds. This study explores the attitudes of caregivers towards dressing of wounds.
Methods: Caregivers of patients requiring dressing of wounds were selected on the basis of inclusion and exclusion criteria. In depth interviews were conducted among 25 selected caregivers after they gave informed consents. Questions included those about details of patients, relation with caregivers, and caregivers beliefs and opinions about the wounds.
Results: Caregivers were wary of the patients’ wounds, their main fear being contagion. Modifiable ones like fear of contagion, revulsion of the wound, and non modifiable barriers like gender and relation of the patient and caregiver.
Conclusions: Some observations made herein run contrary to conventional knowledge about nursing and caregiving in this special condition. Barriers to dressing by caregivers need to be addressed by education and demonstration that wounds become manageable with regular and detailed care.
Oral-11: Knowledge of Hospice and Attitude towards Hospice Admission in Patients with Advanced Cancer in Palliative Medicine Setting in the Indian Sociocultural ContextMuckadenMaryannDeodharJayitaSalinsNaveenChinchalkerGauri GauraiyaDepartment of Palliative Medicine, Tata Memorial Hospital, Mumbai, Maharashtra, India
Background: Despite potential benefits of hospice enrolment, hospice facilities are underutilized among advanced cancer patients. No study has been done which reflects the current knowledge of and attitude of advanced cancer patients receiving palliative care towards hospice in a South-East Asian country.
Aim: To understand knowledge of hospice, attitude towards hospice admission and factors associated with knowledge and attitude among advanced cancer patients receiving palliative care.
Methods: A cross sectional survey was conducted on 75 advanced cancer patients receiving palliative care in Dept of Palliative Medicine, Tata Memorial Hospital, Mumbai using convenience sampling & a specially prepared questionnaire, validated by 5 experts, with 6 questions for knowledge and 10 for attitude (response from strongly agree to strongly disagree). Relevant analysis was done for descriptive statistics. Chi square test was applied to examine associations between knowledge, attitude and different factors.
Results: 25 out of 75 (33.3%) participants had knowledge of hospice. Of them, 68% were aware of presence of doctors and nurses in hospice and 88% knew that end of life care given at hospice. 66.7% participants had no knowledge of hospice and were given brief information on hospice. Analysis of attitude revealed that 7 (9.33%) considered going to stay at hospice meant losing hope. 55 (73.3%) would recommend hospice to others but were unwilling to stay there themselves. 6 (8%) of total were willing to stay in hospice and had low finances or no family support. Higher level of education (p<0.001) and residence in urban areas (p = 0.046) were significant factors associated with knowledge of hospice.
Conclusion: Awareness of hospice is limited among palliative care patients in our study. For improvement of hospice care in developing countries, culturally appropriate educational measures need to be implemented to bring about a positive change in understanding of hospice among palliative care patients & general public.
Keywords: Advanced cancer, attitude, hospice, knowledge, palliative care
Oral-12: Informed Consent in Palliative Care: The Use and Relevance of MultimediaBinoySimoniGhooiRavindra1Department of Communication, Pune, Maharashtra, IndiaDepartment of Cipla Palliative Care and Training Centre, Pune, Maharashtra, India
Palliative care like any other medical treatment must satisfy ethical concepts, such as respect, justice and beneficence. Respect to the patient means giving a choice of therapeutic options but not excluding rejection of treatment. Exercise of freedom of choice makes sense when the choice is made after a thorough understanding of the associated burdens, risks and benefits. At our centre, many of our patients are illiterate, and those who are literate have little understanding of medical procedures. Explaining the concepts of palliative care and procedures that are going to be used becomes an arduous task, to which many of our people are unequal. In western settings there are scales to calculate readability and comprehension of informed consents. In Indian settings we do not have much evidence of the use of such scales. Therefore, it is imperative to innovate the form of delivery of information. The aim is to provide adequate information and educate the patient and relatives about the disease trajectory and procedures before initiating the same. We propose pictorial representation of the procedures as well as multimedia formats to increase understanding and comprehension of patients. Procedures depicted in the form of pictures and videos, are quite easy to comprehend for those with or without knowledge of palliative care. We present PowerPoint with multimedia-based presentations for informed consent to administer epidural analgesia.
Oral-13: Innovation, Learning and Adaptation – The Village and Gram Panchayat ModelBoraSanghamitraDepartment of Palliative Oncology, North East Cancer Hospital and Research, Guwahati, Assam, India E-mail: sanghamitrabk@gmail.com
Background: Generating innovative ideas along with adaptation of successful models of delivery is vital for awareness in the community and creating demand for palliative care. Taking this into consideration a Community Palliative Care Programme has been initiated in the district of North 24 Parganas in West Bengal. Our study is aimed at: (a) Emphasizing the “model village” concept for Palliative Care implementation. (b) Highlighting involvement of the Gram Panchayat to initiate, disseminate and sustain a non-governmental outreach programme.
Method: Under the aegis of MES Medical College and Human care Foundation, a palliative care program was started in Chakla, North 24 Parganas of West Bengal in February 2015. At initiation, a village was chosen where home care was initiated including key persons like village headman, mahila mandal, and youth representatives. Home care and day care services were started. A follow up team reported new patients in the village who reported to the OPD. This was a “model village” for palliative care. The method was replicated in the nearby villages, the effect being reciprocal. One gram panchayat with 22 villages was covered in a span of 4 months.
Result: Two home care teams – doctor led and nurse led; volunteers are rotated weekly in each team. Gram panchayats covered - three. 56 volunteers = 56, 3 doctors, and 8 nurses received basic training in Palliative Care. 456 patients received home based palliative care over the last 12 months including bereavement support for the family. Males = 288; Females = 168; Cancer to Non-cancer patients ratio 110:346.
Conclusion: It can be concluded from the study that there can be successful implementation of community palliative care programs if started at the village level. The community requires motivation and support from technical teams. It is also important to explore palliative care needs in the Non-cancer patients. Basic training for volunteers in this area can help reach many such patients that are underprivileged and difficult to find.
Keywords: Community palliative care; gram panchayat; home care; integration
Oral-14: Change in Adaptive Behaviours of Chronically Ill Children through Psychosocial InterventionKNJanakiPGHariprasad1RajanReeja2Department of Clinical Psychology, SAT Hospital, Thiruvananthapuram, Kerala, IndiaDepartment of Pediatrics, SAT Hospital, Thiruvananthapuram, Kerala, IndiaDepartment of Palliative Care, SAT Hospital, Thiruvananthapuram, Kerala, India E-mail: k.n.janaki@gmail.com
Background: Chronically ill children (Cic) have age inadequate adaptive behaviours due to various reasons.
Objectives: (i) To assess the change in adaptive behaviours of Cic brought on by psychosocial intervention (ii) to assess the perceived stress of mothers of Cic and the influence of the mediators of stress (iii) to assess the perceived psychological distress of the non-disabled siblings (NDS) of these Cic.
Method: A quasi- experimental study of 125 Cic, their primary caregiver biological mothers and their NDSs’; selected based on specific inclusion and exclusion criteria, through consecutive sampling from those attending the Palliative clinic of the department of Pediatrics, of a tertiary care centre. Clearance of institutional ethics committee and informed consent from the participants were obtained. Socio demographic details were collected. Social maturation in eight areas of adaptive behavior and the social quotient (SQ) was assessed at pre- and post psychosocial intervention using the Vineland Social Maturity Scale. The perceived stress and coping of the mothers’ and the perceived psychological distress of the NDS was elicited using semi- structured interview schedules. Intervention comprised; orientation regarding the caregiver mother's stress and coping, supportive counselling, psychoeducation, hands-on behavioural and skills management training for the mothers’ and the NDSs’.
Results: Statistically significant improvement in adaptive behaviours was observed in scores of self help; [general (Δ = 2.56, P = 0.011), eating (Δ = 3.33, P = 0.0001), dressing (Δ = 3.14, P = 0.002), and occupation (Δ = 2.69, P = 0.007), and in SQ (Δ = 2.1, P = 0.0001).
Poor coping in participant mothers’ correlated to higher stress (r = 0.537, p = 0.01) Factor multiple regression identified areas of mediators like awareness (t = 2.02, p = 0.045), child rearing practices (t = 3.53, p = 0.001) and global adaptation (t = 2.53, p = 0.013) as statistically significant parameters mediating stress. Perceived total stress of mothers’ correlated with the NDSs perception of distress on areas like their; awareness needs (R = 0.19, p = 0.034) interpersonal relations with mother (R = 0.325, p = 0.0001), negative experiences (R = 0.266, p = 0.003), school experiences (R = 0.199, p = 0.026), personal emotional experiences (R = 0.235, p = 0.008).
Conclusion: Psychosocial intervention produced significant improvement in adaptive behaviours of Cic.
This study was funded by the Centre for Disability Studies, Thiruvananthapuram.
Oral-16: Enhancing the Quantity and Quality of Palliative Care Volunteers in BangaloreSridharPillalamariTitusSnehaSanman Palliative Care Society, Bengaluru, Karnataka, India E-mail: psridhar360@gmail.com
This is an Action Research project that aims to enhance the number of Palliative Care volunteers in Bangalore, even as it works towards increasing their levels of engagement with patients. The paper describes the usual steps of Action Research, viz. PLAN-ACT-OBSERVE-REFLECT. The researchers noted that the framing of the problem was an insightful process in itself, as this framing resulted in a shift of their position from fitting the volunteer demand to suit the Bangalore population to first understanding Bangaloreans’ lifestyles and consequent availability, and then fitting the demand of volunteers to suit these. As a result, this process allowed the emergence of certain principles that would enable fulfillment of the aim of this Action Research, without making unrealistic demands of potential volunteers, while supporting them as they needed. By conducting interviews across a range of volunteers, a certain understanding of the enablers, constraints, needs, strengths and limitations of likely (as well as not-so-likely) volunteers was arrived at. With this information – and with the set of principles already arrived at - volunteer-induction processes and volunteer support systems were devised and aligned. Where one method of inducting volunteers proved effective, another could well prove ineffective. Such variations were examined and learnt from. Specific indicators of enhancement of quality of volunteering were also arrived at. This paper describes the methods used to understand (and later factor in) the mindsets and felt needs of a range of volunteers, so as to significantly enhance the volunteer base by the time this two-year project is completed.
Keywords: Bangalore, enhancement, palliative care, volunteering, volunteers
Oral-17: Idea of Good Death – Differences between That of the Terminally Ill and the CaregiversSnehaMPalatGayatriDepartment of Pain and Palliative Medicine, MNJ Institute of Oncology and RCC, Hyderabad, Telangana, India E-mail: dreamsorama@gmail.com
Background: Among all branches of Medicine, Palliative care is the only one which is ready to look at the live wire topic that is Death, We, as palliative physicians are trained to not hasten Death or prolong life. With all this how often do we reflect on the idea of ‘Good Death” and do we ever, if at all communicate it? Do the terminally ill person's idea of Good death correspond with what his physician thinks He/she has? How does it affect the quality of treatment rendered? This paper is aimed at assessing the idea of Good Death in the terminally ill and the idea held by the caregivers for the patient at various hospices in Hyderabad and Out patient department at MNJ institute of oncology.
Method: 50 people who are terminally ill and 20 health care providers who care for them, including Doctors, Nurses, Physiotherapists, volunteer and counselors were asked about their idea of Good Death using Death inventory and Quality Of Good Death questionnaire, followed by a focused group discussion. Results were collected, compared, contrasted and analyzed between the two groups and information shared with both.
Results: (1) Only one half of the sample interviewed had thought about good death and less than one third of them had discussed about the same with their physician. (2) That there was a significant different in what the terminally ill wanted in order to call the death experience as Good and what their health care team thought for them. (3) Communication of the results of both the groups did not bring animosity or il feelings as expected. (4) Both the parties reported to have felt more safe and less frustration, misunderstanding and burn out.
Conclusion: This study bring to notice the importance of having the conversation about good death at various points of treatment for the terminally ill and the health care team. It also highlights the fact that communication of differences when realized and shared honestly increases the quality of relationship with the health care providers leading to better compliance, rapport and patient outcome. Patients being the experts in the experience and the Health care providers being experts in the subjects can help each other to make good death possible for the ailing.
Keywords: Death, end of life, palliative care
Oral-18: Caring for the Professional Care Providers: Felt Needs and Challenges in Cancer Palliative Care CentresKaurAmanpreetSharmaMahendra PChaturvediSantosh K1Department of Clinical Psychology, Bengaluru, Karnataka, IndiaDepartment of Psychiatry, NIMHANS, Bengaluru, Karnataka, India
Background: The job of professionals who provide care to terminally ill or dying cancer patients could be both challenging as well as rewarding. Most studies suggest that they are at an increased risk of developing burnout, secondary traumatic stress, and grief. There has been very less work done on developing practical interventions based on the needs and challenges perceived by this population. Thus, it becomes important to study and address these needs as they are the entity responsible for better care of patients and their families.
Methods: Objectives were to explore felt needs of the professional care providers working in cancer palliative care centres and develop an intervention program based on the results. Cross-sectional exploratory methodology was adopted to study the felt needs. Purposive sampling method was used to recruit professionals (doctors, nurses, counsellors, and social workers) from four different cancer palliative care centres in Bangalore who had given the written informed consent for the administration of semi-structured interviews as well as audio recording for the same. The interviews were conducted with five professionals as part of pilot phase of the study. The interviews were transcribed and thematic analysis was carried out using Atlas.ti 6 Software.
Results and Conclusion: Broadly emerging areas on the interviews were: mixed emotions, compassion satisfaction, difficulty dealing with children's death, negative affect and helplessness. The needs, challenges and helpful factors will be discussed in the presentation in detail. Although these are preliminary findings from the pilot phase of the study however the findings are suggestive of need to understand the felt needs of this population and developing an intervention program to promote their personal and professional fulfilment.
Keywords: Cancer Palliative Care Centre, felt needs, grief, professional care providers
Oral-19: Issues Relating to Caring for Patients with Brain Tumours in an Inpatient Hospice SettingSonia LouisMariaKSSundariJohnsonJeremyKarunashraya, Bangalore Hospice Trust, Bengaluru, Karnataka, India E-mail: jeremy.johnson@karunashraya.org
There has been a long-standing belief amongst our counsellors and nursing teams that patients with certain types of brain tumours have higher than usual care needs.
To evaluate this we undertook a retrospective case-note review of all patients with brain tumours, admitted to our in-patient wards between 1st January 2014 and 1st November 2016.
Of the 107 patients, 58 had Gliomas or Glioblastomas, 22 other primary tumours of the brain, and 27 cerebral metastases from a variety of other sites. There were 60 males and 47 females in total.
Of the seven in the paediatric group (ages 5 to 15 years), 2 had medulloblastomas, 2 neuroblastomas, and 3 midbrain or pontine gliomas. Of the three “young adults” 2 had brainstem astrocytomas and one a temporal oligodendroglioma.
The remaining 97 patients ranged in age from 30 to 86 with a median age of 58.
It was found that patients with Glioblastomas had a higher readmission rate, (sometimes with multiples admissions) and a longer average length of stay compared to the rest.
The major influencing factors were:
Poor mobility
Aphasia/dysarthria
Headaches/raised intracranial pressure
Disturbed sleep pattern
Pressure area care
Problems with feeding/hydration
Problems with elimination.
Contributory factors were lack of social and family support and the effect of steroids, leading to weight gain, proximal myopathy, diabetes and restlessness. Not surprisingly, patients with temporo-frontal involvement had greater behavioural and emotional problems.
The impact of these on the nursing and social input are discussed, together with the possible implementation of “Dependency Scoring” to help allocate adequate resources to the patients and their families.
Oral-20: Breaking the Bad News: Guidelines for a Culture Sensitive ApproachBBhuvaneshwariThomasPriya TreesaDepartment of Psychiatric Social Work, National Institute of Mental Health and Neuro Sciences, Bengaluru, Karnataka, India E-mail: priyathomasat@gmail.com
Introduction: Breaking bad news can be defined, as information that “results in a cognitive behavioral or emotional deficit in the person receiving the news that persists for some time after the news is received” (Buckman, 1992; Ptacek and Eberhardt, 1996).
The present paper aims to explore the importance of culture sensitivity in breaking bad news in life threatening disorders.
Culture sensitivity is a major factor in communicating negative news. Cultural factors can determine a patient and their family's belief systems regarding health and illness. The cultural background will determine their outlook towards health care. It also determines their view of death, pain and suffering. If we need to provide quality health care, we must be able to embrace and accept their values and belief system. One-size-fit-all approach will never be effective while breaking the bad news.
Ethnography as a world view, is different than cultural competency. Ethnography emphasizes engagement with others and with the practices that people undertake in their local worlds. It also emphasizes the ambivalence that many people feel because of being between worlds. Kleimann (2008) discuss the ‘explanatory model approach’ as an interview technique to understand how the social world affects and is affected by the illness.
The present paper discusses how this approach can be used to communicate negative information in the clinical settings. This is explored using a case report of working with a child with Duchene Muscular dystrophy and his family.
Conclusion: Based on clinical practice guided by a culturally sensitive approach to breaking the bad news authors put forward certain guidelines for communicating negative information in life threatening conditions.
Keywords: Breaking bad news, communication, cultural factors
Oral-21: Audit of Home Care Service – Timeliness of First Home Visit Post ReferralGargDevinaConsultant, Department of Palliative Medicine, Cansupport, New Delhi, India E-mail: ravindermohan@cansupport.org
Introduction: A clinical audit is performed to improve patient care and outcomes through review of care against set standards and implementation of change. How soon after referral homecare teams visit a patient's home is important because timely reach of support, education and medication to severely ill patients with life-limiting diseases brings relief to patient and family, decreases suffering and hospital visits and leads to a dignified death. This audit was conducted to determine the time within which the palliative homecare teams visited patients after they were referred to the organization and whether the set standard was being followed.
Materials and Methods: Our organization has 25 homecare teams and the audit was conducted for 13 teams. The data was taken from the telephone helpline which keeps records of date referrals are received and date of first visit by homecare teams. The standard set by the organization was 85% of new patients to be visited within 48 working hours of team receiving referral.
The first round of audit was in December 2015 and re-audit was in April 2016.
Results: In December 2015, 96 new patients were registered for the 13 teams. 36 patients were not seen for reasons that were not rectifiable. Subtracting these, total number of patients seen was 60. Delays due to team were 17 making a total of 43 patients seen on time (71.66%), approximately 13% less than set standard of 85%. Main reasons for delay were distance of patient's home from centre, area already visited recently, other end-of-life patients needing frequent visits, holidays and staff on leave. After making changes, re-audit was done in April 2016. Of 58 patients seen, delays were only 6. The standard met was 92%, overshooting the set standard of 85%.
Conclusion: Clinical audits can lead to an improvement in services of an organization.
Keywords: Clinical audit, home care, referral visit
Oral-22: Outcomes among Patients Supported by Specialist Palliative Care Services in Mulago HospitalJTuryahikayo1BMwazi1ENamukwaya1JDowning12MLeng123Department of Medicine, Makerere Palliative Care Unit, Makerere University, Kampala, UgandaGlobal Health Academy, University of Edinburgh, EdinburghCairdeas International Palliative Care Trust, Aberdeen, UK E-mail: mhoira@gmail.com
Background: Makerere Palliative Care Unit (MPCU) is a multidisciplinary hospital based specialist palliative care (PC) service in Mulago National Referral Hospital (MHRH). A novel model of integrated, tiered levels of care which built the capacity of health workers at ward level and offered specialist support has been operating for some time but outcomes were not formally evaluated.
Method: A prospective study carried out in MNRH. All eligible participants newly referred to MPCU were recruited after consent. Socio-demographic data and baseline scores for ECOG and the validated APCA African Palliative Outcome Scale (POS) underpinning physical, psychological, interpersonal and existential domains assessed with 2 reassessments at intervals of 3 days. The ward teams and MPCU continued to offer joint care.
Results: 120 patients were enrolled (117 completed). Spread of diagnosis with commonest cancers hepatocellular (16.7%) cervical (15.8%) and breast (9.2%). ECOG Stage 3 and 4 patients accounted for 41.7% and 42.5% respectively. HIV prevalence was 18.3% with status unknown in 7.6%. Improvement in physical, psychological, interpersonal and existential outcomes demonstrated across the three study visits with statistical significance in median scores. (p<0.001) Differences were seen for participants with complex pain and in the terminal stage (13% and 19% poorer physical and psychological outcomes respectively) and those with higher ECOG (21% poorer existential outcomes).
Conclusion: This study offers important evidence for this model of PC as well as emphasising the role of specialist PC in addressing complex needs. There were measurable improvements in outcome using the validated tools. Patients who had more severe symptoms or who had advanced disease showed overall poorer outcomes as expected. It is important to note that PC is integrated with no separate area for PC and also that patients were seen across the communicable and noncommunicable disease spectrum using a health systems strengthening approach.
Keywords: Health systems, hospital, integration, outcomes, palliative care
Oral-23: Self-monitoring of a Newly Started Palliative Care Clinic at a Teaching Hospital in Rural Gujarat, IndiaKumarDineshDepartment of Oncology and Palliative Medicine, Pramukhswamy Medical College, Anand, Gujarat E-mail: drdineshkl@gmail.com
Background: Our institute is a 550 bedded tertiary care teaching hospital located in a rural area of Gujarat in western India. It has a dedicated cancer centre providing all aspects of cancer care. Palliative care clinic was started at our institute with support of Pallium India from July 2016. We have put in place a simple system to capture data in Excel sheet from the patient’s’ paper record on daily basis.
Methodology: The data was entered into an Excel sheet with inbuilt formulae to calculate various indicators. Some indicators were calculated at the end of every month. The data was entered into the excel sheet everyday by the medical officer or nurse. The current data is for duration July 2016 to November 2016.
Results: Since the beginning of clinic 96 patients were registered with total of 384 visits. Of these only 68 (17%) were females. 352 (91.6%) of visits were due to cancer related diagnosis. The most common symptom was pain 234 (60.9%), followed by wound dressing 127 (33.1%), constipation 35 (9.1%), cough 26 (6.7%), and vomiting 26 (6.7%). 41390 mg of Morphine was used in 53 patients. Per day per capita use of Morphine was 26 mg. 26 (27%) patients had expired. Adjuvants were prescribed in 132 (56.4%) visits. Average duration between palliative care referral and death was 41 days. 34 patients had only single visit to the palliative care clinic.
Conclusion: Continuous capture and analysis of patient data using simple data capture mechanism can help in developing certain indicators related to quality of services in a palliative care clinic. These locally generated indicators can be used for training and sensitization of the other healthcare providers.
Keywords: Health administration, health information system, quality assurance
Oral-25: Effect of Supportive Psychotherapy on Mental Health Status and Quality of Life of Cancer Patients Receiving Second or Subsequent Line of ChemotherapyKMazumderAMukherjeeVKaushalSGhoshalDepartment of Radiotherapy and Oncology, Post Graduate Institute of Medical Education and Research, Chandigarh, India E-mail: koustavmajumder1986@gmail.com
Background: Patients, undergoing second or subsequent line chemotherapy (CCT) often report the presence of anxiety, tension. In this study we intended to find out the mental health status and overall quality of life (QOL) of such patients and to identify the effect of supportive psychotherapy.
Method: 40 consecutive cancer patients undergoing second or subsequent line CCT between April to October 2016, were selected for psychotherapy session. Pre and post psychotherapy evaluation of anxiety & depression was determined by Hospital Anxiety Depression Scale. The QOL (physical health, psychological health, social relationship, and environmental domains) was measured before and after psychotherapy sessions by using WHO QOL Brief Scale. Statistical analysis was done by Paired-t test, using SPSS V.20.
Results: Among 40 patients 17 patients were suffering from Breast cancer and the remaining had Ovarian cancer. All Breast cancer and 19 Ovarian cancer patients were receiving 2nd line CCT. Four Ovarian cancer patients were undergoing 3rd line of CCT. Results indicated that mean scores (± SD) of anxiety (13.95 ± 4) and depression (15.5 ± 4.4) both exceeded the cutoff score of 11 and mean score of QOL physical health (29.77 ± 10.1), psychological health (31.3 ± 10.1), social relationship (35.1 ± 9.6) and environmental condition (25.9 ± 9.9) was below cutoff score of 60. After psychotherapy there was significant improvement of anxiety (P<.01), depression (p<.01) and QOL physical health (P = .02), psychological health (P<.01), environmental condition (P<.01) & social relationship (P<.01).
Conclusion: Supportive psychotherapy helps to reduce the level of anxiety, depression and increase the QOL among the Breast cancer and Ovarian cancer patients undergoing second or subsequent line of chemotherapy. Therefore, psychotherapeutic intervention should be encouraged along with chemotherapy to promote positive mental health and to obtain full benefit of their physical treatment.
Keywords: Chemotherapy, quality of life, supportive psychotherapy
Oral-26: Play Therapy in Pediatric Palliative CareRVineelaPalatGayatriJacobJeanMPavitra1LKumar1Department of Pain and Palliative Medicine, MNJIORCC, Hyderabad, Telangana, IndiaDepartment of Pediatric Palliative Care, Pain Relief and Palliative Care Society, Hyderabad, Telangana, India E-mail: vineela.rapelli@gmail.com
Background: MNJ Institute of Oncology & Regional Cancer Centre is one of the few centres in India to have a dedicated pediatric palliative care program for children with cancer. Our dedicated team provides palliative care to about 350 new children and more than 3000 reivew children with cancer every year. Children undergoing cancer treatment in India usually have to drop out of school and be separated from their siblings and friends. In the hospital wards, they seem withdrawn, anxious, and irritable most of the time while undergoing long treatments and traumatic procedures. Our counselors sit at the bedside of the patient and try to talk to him or her about cancer and what they understand. Often the child's emotional and psychological suffering remains hidden. We believe that no child should suffer or forget how to laugh and play.
Methods: To help these cancer patients be like children again, we started a pilot project to incorporate play therapy into the pediatric palliative care program over a one-month period. Play is the “work”of childhood and it is important for them to reach their developmental goals. A certified play therapist worked with the children for two hours a day for two days a week. The therapy included both group and individual sessions and involved various modalities such as color therapy, play dough, story-telling, craft work etc.
Results: Play therapy helps kids express feelings, encourages creative thoughts and new ideas, encourages development of healthy decision making skills and enables communication. During the play sessions we discovered that children expressed fear and anger about their disease and its treatment which they had not spoken to the counselors about. In that familiar environment of make-believe and imagination, the play therapist was able to elicit the hidden thoughts and emotions of children living with cancer in India.
Conclusion: Play therapy activates the child's innate self-healing abilities, supporting the child's growth and development on an emotional and psychological level. Children can act out feelings or actions that scare them, anger them, hurt them, and work out solutions. Play is the way children learn some of their socialization skills. This is the way they make sense of their life experiences. Adults talk; children play it out!
Keywords: Communication, play therapy, pediatric palliative care
Oral-27: Spiritual Distress among Indian Caregivers in Paediatric Palliative Care Setting – A Qualitative StudyKVGanpathyMuckadenMary AnnSalinsNaveenDepartment of Palliative Medicine, Tata Memorial Hospital, Parel, Mumbai, Maharashtra, India E-mail: ganpathykv3@gmail.com
Advanced illness coupled with imminent mortality of the loved ones can be one of the facilitators for caregivers to pursue spiritual meaning. Some struggle with their relationship with God, some feel their faith shaken out completely. Thus spiritual pain becomes a significant part of suffering and the Impending death contributes immensely to the caregivers’ spiritual distress. There are very many studies that posit importance of Spirituality & religion to the well-being of cancer patients and caregivers. However, spiritual distress of caregivers in the paediatric palliative care setting in India, have not found much mention in the literature.
Research Question: Exploring the spiritual distress among Indian caregivers accessing pediatric palliative care services.
Methodology: The study included 20 eligible parents, accessing outpatient palliative care services, purposively recruited. Either of the parents were interviewed. Interviews were recorded and transcribed. The transcripts were thematically analyzed.
Results: Following themes emerged out of the interview [Table 1].
Themes from the interview
Conclusions: Indian caregivers of paediatric palliative care experience a significant level of spiritual distress that is commonly expressed in the form of anger, being betrayed and punishment by god.
Oral-29: Disseminating Research into Practice: Early Palliative Care VideoSAMurrayGMitchell1SMoine234JAmblà s-Novellas56BoydKirstyPrimary Palliative Care Research Group, The Usher Institute of Population Health Sciences and Informatics, Medical School, University of Edinburgh, Edinburgh, ScotlandFaculty of Medicine, University of Queensland, Brisbane, Queensland, AustraliaMulti-professional Group Practice “The Vines of the Abbey”, 60130 Saint Just en Chaussée, FranceHealth Education and Practices Laboratory, University Paris 13, ParisSimUSanté, Amiens University Hospital, Amiens, FranceDepartment of Geriatric and Palliative Care, Hospital Universitari de la Santa Creu and Hospital Universitari de Vic, SpainChair of Palliative Care, University of Vic, Barcelona, Spain E-mail: Morag.Edwards@ed.ac.uk
Background: Early palliative care may prolong life as well as improve its quality. But many clinicians and patients are not aware that palliative care can be very helpful from an early stage. Clinicians are often not aware of research findings due to poor dissemination. We thus set out to disseminate a rationale for early palliative care for people dying with different conditions. We aimed to make students, GPs and hospital doctors aware in a simple accessible way of when and how palliative care might be integrated with disease modifying care for different conditions.
Methods: We constructed a 4 minute video creatively showing how physical, social, psychological and spiritual needs vary at the end of life for different typical trajectories of physical decline. We did this for the acute (cancer) trajectory, the intermittent trajectory of organ failure, and for the gradually declining one of frailty or dementia. We based this on a secondary analysis of 16 serial interview studies we had published in the last decade. We created images to help us describe display and communicate patterns of well-being and distress felt by people with advanced cancer, organ failure and frailty. We showed these videos in medical schools and at conferences.
Results: We will play the 4 minute video. Previously students have enjoyed the learning experience. Many attendees at the conferences said they would like copies of the video to use to teach clinicians and students, and share with colleagues. Others suggested making a copy to use to explain these issues to patients and carers. The UK Open University want to use the video.
Conclusions: Brief entertaining digital presentations may be effective in communicating and disseminating research findings, and be useful in teaching. A core competency of researchers should be effective dissemination. Creative approaches may also raise public awareness of palliative care.
Oral-30: Palliative Surgery in OncologyRMohanrajV N Cancer Centre, G Kuppuswamy Naidu Memorial Hospital, Coimbatore, Tamil Nadu, India E-mail: mohanraj@gknmh.org
Primary aim of the palliative surgery is to relieve the symptom and improve the quality of life of the patient. Areas of concern are Airway obstruction, bowel and biliary or urinary obstruction; Bleeding from oral, soft tissue, fungating breast cancers and gynaecological cancers; Large tumours in the limbs with severe pain; Perforation of a viscous in the abdomen. Most of the time patient will be having combination of these symptoms. Assessment of the Patient is important to perform the surgical procedure. Performance status of the patient should be good (KPS > 50%), patient's expected survival should be at least 3 months, success of the procedure and durability of the symptoms resolution should be good. One has to consider the availability of the Non surgical methods and Cost effectiveness of the procedure. Palliative surgery is difficult than a curative surgery. It needs high level judgment and expertise. Sometimes not to perform a surgery is a wise option. Care must be individualized in a multi disciplinary manner that is appropriate for a specific patient. Ideally palliative surgical procedure should not have morbidity and mortality. Tracheostomy for airway obstruction, External carotid ligation for a bleeding cancer of the oral cavity and oropharynx, Self expanding stents for dysphagia due to esophageal cancer, Percutaneous gastrostomy for a oropharyngeal cancer, Feeding jejunostomy for a hypo pharyngeal cancer, excision and primary closure or with local flap for fungating cancer of the breast and soft tissue cancer of limb and trunk, Amputation of the limb for large painful cancer of the extremities, colostomy for large bowel obstruction, recto vaginal fistula or severe bleeding from radiation proctitis are common palliative procedures. Fractures of the long bones and vertebrae can be fixed if the longevity of the patient is reasonable.
Oral-31: Assessment of Probable Neuropathic PainSenNagamaniBhagatSurbhiSumathiThenmozhiDepartment of Pain, G Kuppuswamy Naidu Memorial Hospital, Coimbatore, Tamil Nadu, India E-mail: drnagamani@gknmh.org
Aim: To assess the relevance of Douleur Neuropathique in 4 questions (DN4) and Leeds assessment of neuropathic symptoms and signs (LANSS) scoring system in suspected neuropathic pain.
Methods: This prospective observational study was carried out in GKM Hospital pain department during the period september 2015 to october 2016. 732 patients with the complaints of pain were seen in the pain out patient clinic.51 of these 732 patients were diagnosed as having probable neuropathic pain from the history of type of pain, objective neurologic sign or history of definite neurological lesions. They were assessed by two type f scoring tool namely DN4 and LANSS score.
Results: Of the 51 patients with probable neuropathic pain 17 patients were deemed positive by the screening tools. DN4 was positive in 15 patients, and 2 patients by LANSS. One patient was positive by both scores. These patients were now labelled as probable neuropathic pain and treated as such.
Conclusion: DN4 scoring gives a higher number of patients as compared to LANSS. Therefore DN4 scoring tool is more useful in diagnosing probable neuropathic pain.
Keywords: Neuropathic pain, LANSS, DN4
Oral-32: Nurses’ Concerns Following the Introducing and Implementation of a Care Plan for the Dying PatientLouisMaria SoniaJohnsonJeremy RKarunashraya, Bangalore Hospice Trust, Bengaluru, Karnataka, India E-mail: jeremy.johnson@karunashraya.org
A consensus meeting of several Palliative Care providers from around the country led to the formation of “Project India” and the adoption of the principles agreed by the International Collaborative for Best Care of the Dying Person.
Karunashraya, an independent hospice, was given the task of designing an End of life Care Plan (EOLCP) that embodied the concepts, and to test it for feasibility in an inpatient setting.
Crucial to the success of implementing such a care plan was to ensure complete involvement and agreement of all the nursing staff. Initial discussions revealed the following significant concerns:
Doubts regarding the practical feasibility
Increase in amount of paper-work
Reluctance to change current practice
Although recognising a patient was dying, mistrust in their own ability, leading to reticence in verbalising their feelings in a multidisciplinary team discussion
Fear that in acknowledging it, that they were “sentencing” the patient or hastening death
Difficulty in discontinuing unnecessary medications or nutrition
Unease in stopping, irrelevant, routine observations; eg: BP, Pulse, Temperature
Discomfort in explaining this to relatives (particularly out-of-hours).
Numerous discussions and education sessions regarding the concepts of what was being attempted were needed in the initial phases. Feed-back with regard to the wording and structure of the documentation was taken seriously and incorporated into a final user-friendly version. On-going training sessions helped allay further queries and doubts. Since mid-May, some 170 patients have been enrolled into the EOLCP and the notes being audited and tested for congruence.
Outcomes: Several recent focus-group meetings with all the nurses (>70) have revealed an increase in their:
Knowledge
Job satisfaction
Ability to discuss concerns with other team members
Confidence in discussions with patients and relatives
More efficient record-keeping
Sense in Project ownership
Keywords: End of life care plan, nurses’ concerns, project implementation, staff education
Oral-33: Factors Affecting Medication Compliance in a Home Care SettingAgarwalRadhikaJohnsonJeremy RKarunashraya, Bangalore Hospice Trust, Bengaluru, Karnataka, India E-mail: jeremy.johnson@karunashraya.org
Background: Adherence to therapy is the main determinant of treatment success. Failure to comply with prescribed medication often leads to poor symptom control or worsening of disease, with consequent major impact for patient and carers. Whilst it is easy to monitor dispensing and consumption in an in-patient hospice ward, the same is not the case in the community. This study was therefore undertaken to examine factors affecting medication compliance in the home setting.
Method: Following informed consent, 25 patients coming into the hospice from home (most for the first time), were surveyed, together with a further 16 currently undergoing home care. All patients had advanced cancers and were from Low or Middle Income Groups. One-to-one interviews were conducted with the person responsible for the medication, be it patient or carer. The MMAS-4 survey was chosen as it was available in Kannada and valid across all literacy levels.
Results: Compliance was significantly worse in those patients not seen by the Home Care Teams. Reasons for this include: (1) Poor understanding regarding the purpose and timings of the medicines. (2) Barriers to access (cost/distance/pharmacy). (3) Adverse side effects. (4) Contrary advice from family members or other doctors. (5) Lack of social support (particularly elderly patients). Only one patient (with a supraglottic tumour) reported difficulty in swallowing medication. In the unsupported group, there was better compliance in patients in the Middle Income Group though there was no difference seen in patients receiving regular Home Care. It was not possible to correlate education level with compliance as most patients were illiterate.
Conclusion: Patients under Home Care teams benefitted from ongoing monitoring, education and access to regular medication. For those beyond the geographical catchment, we have instituted regular telephone follow-up, information leaflets and recording of daily logs.
Keywords: Compliance, home care, medication
Oral-34: The Multidimensional Experiences and Needs of Ugandan Heart Failure Patients over Their Illness CourseNamukwayaElizabeth1GrantLiz2DowningJulia12LengMhoira123MurrayScott A4Makerere University College of Health Sciences, Kampala, UgandaGlobal Health Academy, The University of Edinburgh, EdinburghCairdeas International Palliative Care Trust, Aberdeen, UK E-mail: mhoira@gmail.comPrimary Palliative Care Research Group, The University of Edinburgh, Edinburgh
Background: Successful management of advanced chronic diseases should be multidisciplinary and should include palliative care (PC) that is informed by the patients’ experiences and needs. However, there is little information on Heart Failure (HF) patients’ experiences and needs in Africa which represents a different pathological, clinical and social spectrum. The aim of this study was to understand the multidimensional experiences and needs of Ugandan HF patients over their illness course so as to develop patient-centred PC for this increasingly prevalent group of patients.
Methodology: HF patients were recruited in Mulago National Referral Hospital (MNRH) and serial qualitative in-depth interviews conducted at 3 time points (at first contact, 3 months and 6 months) over 6 months. A grounded theory approach was used in the analysis. Ethical approval was obtained from the MNRH Ethics committee and the Uganda National Council of Science and Technology and written consent was obtained from participants.
Results: 48 interviews were conducted. The patient's experience was that of learning to live with the unknown in a life dominated by symptoms. The trajectory of functional and social decline mirrored the increasing symptom burden. Other themes included; a high level of health illiteracy, lack of information on their illness, high reliance on local cultural beliefs to make health decisions and health system challenges. The illness impacted the social, psychological and spiritual domains of patients’ lives leading to multidimensional needs. Available services did not meet all patients’ needs.
Conclusions: This study identified similar themes in the multi-dimensional experiences and needs of HF to those in high income countries but also identified themes less common in the literature that led to different experiences. Cardiology teams should be encouraged to integrate PC in their clinical care so that all dimensions of need are addressed.
Keywords: Experiences, heart failure, palliative care needs
Oral-35: Extending Effective Palliative Care to Chronic Kidney Disease PatientsWarrierJyothi JayanEDivakaranInstitute of Palliative Care, Pain and Palliative Care Society, Thrissur, Kerala, India E-mail: edivakaran@gmail.com
Background: Advances in health care delivery have extended life expectancy in renal patients. But they do not restore quality of life. The emotional cost for long term treatment is also overlooked in medical care. There is opportunity to offer effective palliative care to patients struggling with issues connected to this non-malignant disease. Objective -To assess, whether the palliative care services provided by our organization, to the renal patients on haemodialysis, was bringing about any significant change in their quality of lives.
Method: 25 renal patients on haemodialysis, registered with our palliative care society for more than a year, were randomly selected. Their quality of life was assessed using the structured questionnaire KDQOL – SF Version 1.3 by RAND. This was compared with the quality of life measures of 25 patients who receive no palliative care support. The 36 items of RAND help to assess six domains viz, physical functioning, role limitations, emotional well being, social functioning, energy and pain of renal patients.
Result: A comparative study was conducted and data analysed using statistical measures. There was no statistically significant change in the quality of life of patients who were registered with our palliative care society.
Conclusion: The renal patients are by and large hidden patients. Usually caregivers visit our clinic, get free medicines and receive emotional support. It is taken for granted that the issues of renal patients are addressed by the nephrologists. However, the nephrologists, fail to look into and effectively manage, the suffering caused by the incurable nature of this illness and the associated distress that are beyond lab values. So there is a need for palliative care workers to take proactive role in the care of patients with End Stage Renal Disease.
Keywords: Chronic kidney disease, haemodialysis, palliative care, quality of life
Oral-36: A Qualitative Study on Palliative Needs of Stroke Patients in an Indian Tertiary Care Setting – Doctors’ PerspectiveLloydJacobPintoAshnaNairShobaTareySubashDepartment of Palliative Medicine, St. John's Medical College, Bengaluru, Karnataka, India E-mail: nair.shoba@gmail.com
Introduction: Stroke is the development of a focal neurological disturbance lasting more than 24 hours, of vascular origin. In India, stroke is one of the leading causes of morbidity and mortality. Most stroke patients, during their duration of treatment and post hospitalisation, want relief of suffering, a sense of control and minimised burden on family.
Objective: To describe treating doctors’ perspectives on the palliative needs of stroke patients in India.
Methodology: This qualitative study was done in a tertiary care hospital in South India. 17 doctors involved in the care of stroke patients were interviewed, using an interview guide. The interviews were audio recorded simultaneously. The audio recording was transcribed verbatim and the data was coded using a grounded theory approach. An inductive approach using thematic analysis was used to manually analyse the data.
Results: Eight themes emerged. (1) Functional disability: Loss of independence due to immobility, speech deficits, visual disturbances, feeding difficulties and incontinence causes immense distress. (2) Physical burden: Pain in the form of Central post stroke pain, periarthritis shoulder, psychogenic pain and various sequel of chronic bed bound state like bedsores and pneumonia add to the burden. (3) Psychological needs: Depression is common in stroke patients along with other psychological issues like anxiety, agitation, apathetic state and behavioural disturbances (4) Social issues: Cost of treatment of stroke patients coupled with their loss of employment leads to huge economic burden. They also face abandonment by children or spouse, in all sections of socioeconomic strata. (5) Caregiver burden: Caregiver has a major role in a setting of stroke and in the long term affects all domains of their lives, compromising their psychological and physical health. (6) Counselling-an unmet need: Counselling is particularly important in a setting of stroke for the patient as well as the caregivers and results in a better patient outcome. However, clinicians expressed that it was inadequate due to the huge patient load, time constraints and lack of effective counselling skills. (7) Spiritual needs: Few clinicians stated that existential distress and spiritual struggle are seen in debilitated stroke victims and are often unaddressed. (8) Issues at end of life care: Patients with massive stroke, multiple co morbidities and poor rehabilitative potential requires end of life care.
Conclusions: From the interviews of the clinicians, we can conclude that care of a stroke patient is more than medical management and rehabilitation, as several other aspects of the patient's life is affected by the condition. The quality of life aspect has to be looked upon as an area that requires active intervention in a setting of stroke. Physical disabilities were viewed as the most significant factor reducing the quality of life. Spiritual needs have a low priority in comparison to other physical needs. Due to high patient load and time constraints, many of the needs are unaddressed. Two important areas where palliative medicine has a major role in a setting of stroke are counselling and alleviating caregiver burden. However referral of stroke patients to palliative medicine is low and further research to identify barriers to specialist palliative care of stroke patients will help in promoting the referrals to palliative medicine.
Keywords: Care, needs, palliative, stroke
Oral-37: Working for Palliative Care: The Inner Journey of Palliative Care ProfessionalsThatteNandini NNaikVinay ADepartment of Research and Training, Cipla Palliative Care and Training Centre, Pune, Maharashtra, India E-mail: nandini.thatte@gmail.com
Background: Working with pain and suffering every day, is difficult. Yet a compassionate few choose to make it their life endeavor. The nature and experiences from one's work do influence the individual and his own way of life. It helps build the resilience demanded by this profession. Understanding this process would help building support systems for existing professionals and also, aid the induction and retention of new professionals in the mentally demanding field of palliative care.
Method: This study traced the inner journey of ten palliative care professionals working in Pune, India. The narratives were recorded, transcribed and analyzed.
Results: The narratives were analyzed to explore underlying themes and delved into their journey from Introduction to Palliative Care, Career decisions, Motivation, Challenging scenarios witnessed and Coping with mortality. The interviews gave an insight into the impact of Palliative Care in reshaping perspectives of these individuals to view life in a new light.
Conclusion: The results gave an insightful picture of how these professionals trained themselves in and adapted to the demands of palliative care service delivery. It was found that work experiences significantly impacted the professionals’ perception of life, personal lifestyle, and beliefs about life, death and disease. More professionals from varied settings need to be interviewed to collate more generalizable conclusions.
Keywords: Coping, motivation, palliative care
Oral-38: Treatments Given to Patients in the Last Month of Their Lives at a Regional Cancer Center in IndiaJacobJeanPalatGayatriKaurJaskirt1MPavitra2LKumar2Department of Pain and Palliative Medicine, MNJ Institute of Oncology and RCC, Hyderabad, Telangana, IndiaDepartment of Pediatric Palliative Care, Pain Relief and Palliative Care Society, Hyderabad, Telangana, IndiaMedical Student, Lund University, Lund, Sweden E-mail: jeanjacob82@gmail.com
Background: The MNJ Institute of Oncology and Regional Cancer Center in Hyderabad (MNJIORCC) provides cancer treatment and palliative carefree of cost to underprivileged patients. Aggressive tumor-specific treatment (chemotherapy and/or radiotherapy) at the end of life has been proved to offer no improvement in survival or quality of life and the practice has been abandoned in developed countries in favor of supportive and palliative end of life care. However, in India, it is still common to have chemotherapy and radiotherapy continued in the last few days of a patient's life, thereby adding needless suffering to their end of life, often without the support of palliative care. There is little awareness about this problem in India.
Method: The purpose of this study was to describe the treatments given in the last month of life to adult patients with cancer at MNJIO&RCC. Data was collected from the last 2 months (April and May, 2016) of patients between the ages of 18 and 80 years who died while undergoing treatment at the oncology department of this hospital. It was determined to what extent tumor-specific treatment was given in the last month of life and how close to the day of death it was continued. It was also determined how many of these patients who died in the hospital had been referred to the palliative care department in their last month and what symptoms they were referred for and what treatments were given.
Results: A total of 55 adult patients died at MNJIO&RCC in April and May, 2016. Their ages ranged from 19 years to 80 years and mean age was 44 years. Most common diagnosis was acute myeloid leukemia, followed by lung cancer and breast cancer. 75% of the patients who died were receiving tumor specific treatment. Of that number, 95% received tumor-specific treatment in the last month of life. 63% received tumor-specific treatment in last week of life and 27% received it on the day they died or the day before. 49% of these patients were referred to palliative care in their last month of life. Most common reason for referral was pain, and 70% of those referred received morphine.
Conclusion: The data revealed that a majority of the patients at MNJIO&RCC receive tumor-specific treatment in the last few days of life. This adds needless suffering to their end of life. Only about half of these patients get referred to the palliative care department. Awareness needs to be spread to cancer healthcare providers and to the public regarding this issue so that futile aggressive tumor-specific treatments can be abandoned earlier and instead more palliative care can be offered to these patients at the end of their lives.
Keywords: Cancer, end of life treatment, palliative care
POSTER PRESENTATIONS: PP/10/01: Seeking God in a Time of Grief: A Personal PerspectiveSinghAbhinavDepartment of Palliative Care, Jeejeevisha Niketan, Samastipur, Bihar E-mail: lionabhinav@yahoo.co.in
Background: In monotheism, God is conceived as Supreme Being and principal object of faith. At the end of life, as a doctor we have dual responsibility to preserve life and relieve suffering. During suffering a religious person might ask “where does my help come from? My help comes from Lord, the maker of heaven and earth” (Psalms 121:1,2). By the time patient visits a palliative physician he/she may hopeless, helpless, confused with lots of superhuman expectations.
Methods: To reflect on patient's grief and his expectations and the response of doctor in such situation.
Observation: Patients sometimes say “Doctor you are God on earth! Please help!” In such situation we can either say ‘sorry’ and escape or respond by journeying at his pace on the path of spirituality. There are multiple examples from various religions and cultures where communication at the level of spirituality decreases uncertainty, enhances relationship. Proper communication from palliative care provider helps patient accept truth and plan his future course of action with realistic optimism.
Conclusion: A doctor should guide patient in struggle for survival and “perform his prescribed duty”. (Bhagavad Gita, Chapter 3 verse 8). During appointment with patient, doctor should keep in mind “without being attached to results of activities one should act as a matter of duty.” (Karma Yoga, Bhagavad Gita). It may not happen so quickly in many cases.
Keywords: Communication, end of life care, spirituality
PP/10/02: Factors Influencing the Initiation of Strong Opioids in Cancer Patients on Palliative Care: An Audit from a Tertiary Cancer Centre in IndiaBParmarRMiriyalaMAHurriaSGhoshalDepartment of Radiotherapy and Oncology, RCC, PGIMER Chandigarh, India E-mail: parmar.bhushan@gmail.com
Background: A significant proportion of cancer patients on palliative care require some form of analgesia. However need for strong opioids in these patients is inconsistent and unpredictable.
Objectives: To evaluate the factors influencing initiation of strong opioids and duration of their use in palliative care patients.
Methods: Case records of 187 patients registered for palliative care at our centre between January and April 2015, were retrospectively analysed. Factors influencing initiation of strong-opioids and duration of strong-opioid free interval were evaluated using multivariate analysis.
Results: Median age was 55 years. 60% of the patients were male; 40% were female. 84.5% of the patients had pain, while only 16% required strong opioids like morphine or fentanyl. Radiation was given for palliation of pain in 65% of patients. Median duration of treatment with strong-opioids was 47.5 days, while median morphine free interval was 29 days. Age of the patient, stage at diagnosis and requirement of weak opioids at the time of registration had significant correlation with initiation of strong opioids (p<0.05). Marital status of the patient, income, disease burden at the time of palliative care registration and use of palliative radiation had significant impact on the duration of strong-opioid free interval in our study.
Conclusion: Use of strong-opioids for adequate analgesia is not a necessity for all palliative care patients. Optimal utilisation of adjunctive analgesic modalities like radiation, coupled with good supportive care can minimize the requirement and duration of strong-opioid use, especially in developing countries with limited access to specialist palliative care.
Keywords: Prescription, opioids, palliative care
PP/10/0: Psychological Distress in Patients in End Stage Renal DiseaseJithAryaVenkateswaranChitraDepartment of Psychiatry, Amrita Institute of Medical Sciences, Kochi, Kerala, India E-mail: aryaji2008@gmail.com
Background: Chronic Kidney Disease has been increasing worldwide so is the number of patients undergoing maintenance haemodialysis. They have high prevalence of psychiatric co morbidity which remain undiagnosed. Aim of my study is to assess psychiatric co morbidity in End Stage Renal Disease patients undergoing maintenance haemodialysis.
Method: This is a cross-sectional Study enrolled 110 patients >18 years on maintenance haemodialysis. Psychiatric co morbidity was assessed using M.I.N.I International Neuropsychiatric Interview version 6 (Malayalam).
Results: Out of 110 patients 67.3% had depressive symptoms and 60.9% had anxiety symptoms in M.I.N.I. The prevalence of all other psychiatric co morbidity was less. It was also found that suicidality was also associated with depression and anxiety symptoms.
Conclusion: Depression and Anxiety are the most common psychiatric disorders in end stage renal disease. These are all treatable conditions which can improve the quality of life of these patients. So it is important to diagnose and treat these conditions. The high prevalence of emotional and psychological symptoms in these patients should alert the nephrologist and palliative care team.
Keywords: Anxiety, depression, end stage renal disease
PP/10/05: Assessing Resilience and Quality of Life in Caregivers of Advanced Cancer PatientsSinghaiPankajDepartment of Palliative Medicine, Tata Memorial Hospital, Mumbai E-mail: doctorpsinghai@gmail.com
Methods: Study design: Cross sectional Observation study. Setting: Department of Palliative Medicine, Tertiary Cancer Centre. Population: Primary caregivers of patients with advanced cancer referred to Department of Palliative Medicine.
Results: 75 caregivers were enrolled for study, 71 completed questionnaire. Mean age of patients was 54 years (SD – 15.92), Mean age of caregivers was 36.51 year (SD- 11.61). Mean Resilience Score was 70.17 (SD- 16.49, Range 19.31-100). WHO QOL (Quality of life) scores of different domains were Physical Health domain: 59.18, Psychological wellbeing domain: 57.84, Social relationship domain 68.89, Environmental domain 56.21, Overall domain 66.54. Pearson Correlation coefficient resilience score with different domains of QOL were 0.293 with Physical Health domain, 0.419 with Psychological wellbeing domain, 0.374 with Social relationship domain, 0.420 Environmental domain, Overall domain 0.461.
Discussion: Resilience score of cancer patient's caregiver were lower than that of general population (US) (Connor and Davidson (2003)); were comparable with caregivers of Bipolar disorder (Jain A 2014) and better than care givers of Schizophrenia and Dementia. Correlation between resilience score with different domains of QOL was moderate to weak.
Conclusion: The resilience of caregivers of advanced cancer patients is comparable to caregivers of other illnesses. Resilience is correlated with quality of life (weak to moderate).
Keywords: Care giver, palliative care, resilience score
PP/10/06: Impact of a Public Awareness Program in Palliative Care: A Model Project by Pallium IndiaAbrahamBabuMattamAnnDepartment of Palliative Care, Pallium India, Thiruvananthapuram, Kerala, India E-mail: babu@palliumindia.org
Introduction: Pallium India is a national registered trust, based in Trivandrum aiming to provide and establish quality palliative care services and pain relief for patients in India through service development, education, research and advocacy. Current public awareness of the concept of palliative care and of the services available remains insufficient for widespread acceptance or service uptake. This has huge implications for palliative care service provision and policy. A comprehensive assessment of public awareness regarding palliative care is therefore required in order to design and implement appropriate interventions. An increased awareness is required in order to empower individuals, encourage community engagement and to improve knowledge of and access to palliative care services.
Objectives: (1) Study the impact of public awareness events. (2) Review how many new volunteers and community groups are recruited or formed as a result of training. (3) Assess the impact on patients.
Materials and Methods: As a part of Pallium India's advocacy work, a team was created with the aim of raising public awareness. The team (consisting of trained volunteers, social workers, nurses and doctors) sought out audiences at locations around Trivandrum such as residence associations, schools, colleges and corporate headquarters. After audiences were identified a program was conducted following a specific curriculum. This study evaluates the programs held between January and November 2016 (a total of 65 events). Feedback was collected from participants through voluntary semi-structured telephone interviews, focusing on the understanding of palliative care, recruitment of new volunteers; emergence of new community groups and how many new enquires regarding services were received.
Outcomes: (1) This study reveals steadily increasing awareness regarding palliative care. (2) Positive reactions towards palliative care by the public were demonstrated by new volunteer recruitment and new community group formation. (3) Increased numbers of enquiries about our palliative care services. (4) Increased financial support. (5) Improved quality of services for patients.
Conclusion: This study supports the positive impacts of public awareness programs in changing public perceptions in order to further improve attitudes and service provision of palliative care.
Keywords: Education, training, volunteer
PP/10/07: The Need and Necessity of Spiritual Counselors in Palliative Care SetupDBhoopathy1ThomasNaveen2Counselor and Volunteer, Karnataka, IndiaDirector, Bangalore Baptist Hospital, Bengaluru, Karnataka, India E-mail: naidums2003@gmail.com
Aim: To make one to understand the power of one's own spiritual strength to cope up with the cancer disease trauma in life. To make them aware of it's use as a therapeutic tool and also practice as conscious based medicine for the redressal of the end stage patient.
Background: General public relate spirituality to religion. It means to realize one's own faith in God or rise themselves to higher consciousness, as well as to know and experience one's universal connectivity with God and other beings. All terminally ill patients’ irrespective of their faith & religion aspire for good death. All patients irrespective of the stage of their disease no matter what their faith and beliefs of religions are, need spiritual care to cope with the disease. Christian pastors regularly visits the terminal patients in various hospitals (BBH, KMIO.CSIH), hospice and care centers compared to other religious leaders.
Method and Tools: With oral questionnaire was prepared and presented to two doctors and eight hospitals patients (BBH, KMI O&MSR), to find out their knowledge, understanding and the necessity of spiritual therapies and its benefit in pain relief. To assess their pain level before and after prayers and spiritual counseling, Johns Hopkins pain rating Instrument (numerical scale) was applied.
Results: (1) With regard to Doctors: (i) 60% believes in spiritual care. (ii) 80% understands that spirituality is related to humanistic value. (iii) 40% feels the necessity of the spiritual counselors in the palliative team. (2) Patients: (i) 80% of the end stage patients want prayers for their well being. (ii) 70% needs spiritual counseling. (3) After prayer and meditation, there is difference of 2% less pain as per the pain scale reading.
Conclusion: Spiritual understanding gives strength to fight the disease. Prayers & meditation acts as conscious based medicine in bringing down their stress levels. There is no static research data with regard to quality of life measured by linear Analogue assessment scale nor spiritual distress pain assessed by Edmonton symptom assessment spirituality (ESAS). Spiritual understanding and counseling helps in creating a good networking system between the caretakers, community members, social workers and helping groups to connect with patients. There is a spiritual lacuna in the health system because of lack of spiritual infrastructure and lack of psycho social spiritual role module in the hospitals and medical care system.
Future Need: Every hospital's palliative care team should have a regular spiritual counselor and have spiritual clinics to assess patient's spiritual distress. Urban district level hospitals should have spiritual clinical cell with trained, experienced and skilled counselors and health workers to handle inter and intra multi religious patients. Let spirituality be a friend in deed to the patient. The goal is make “spiritual access for pain control to be seen as the right of all cancer patients at any stage of their disease.” Spirituality is the sacred thread that passes through all regions of humanity, binding humans together. Spirituality prepares the dying patients to “Sing your death song and die like hero going home” (Tacunnseb Shawanne).
Keywords: Spiritual care, spiritual counselors, spirituality
R<sc>EFERENCES</sc>PuchalskiCMFerrellBOtisSOverview of Spirituality in Palliative CareLast accessed on 2016 Oct 20Available from: http://www.Green.uptodate.comBroeckaertBSpirituality and palliative careIndian J Palliat Care2011173941PP/10/08: Electrochemotherapy: An Effective Palliative Measure for Superficial Localised LesionsMathewAsokeTiruvadananMallikaMuthukumaranSubathraPalliative Care Unit, Lakshmi Pain and Palliative Care Trust, Lakhmi Sundaravadanan Hospital, Chennai, Tamil Nadu, India E-mail: lakshmipaincare@gmail.com
Objective: To reduce pain and tumour size and promote healing of malignant wounds using Electrochemotherapy in inoperable, recurrent, and radio and chemoresistant cancers not responding well to current standards of cure.
Method: There is critical need for a safe, yet affordable, alternative physical treatment which is effective for the treatment as well as palliation of symptoms of various types of localised cancers.
Electrochemotherapy is one such treatment modality used in our clinic. It is an efficient technique to enhance drug delivery to the tumour cells by electroporation.
Electro chemotherapy involves the local application of pulses of electric voltage to tumour tissue, to render the cell membranes permeable which are otherwise poorly permeable to anticancer drugs thereby facilitating a potent localised cytotoxic effect.
Intracellular concentrations of bleomycin are increased 1000 fold resulting in cell death by apoptosis-like phenomenon. There is very little injury to the normal surrounding cells and tissues and inflammatory reactions are minimal.
Two female patients presented to us with sarcoma in the lumbosacral region. They had local tumours, pain and were unable to lie down on the back. They had undergone surgery, chemotherapy or radiation ECT was done in the theatre under light sedation. A small dose of Bleomycin (10 mg) was given IV and followed 10 min later by ECT. It can be done as a day care procedure.
Conclusion: Both patients had relief of pain as there was a marked reduction in the size of the tumour. Electroporation mediated chemotherapy, known as Electrochemotherapy (ECT) is a viable alternative palliative treatment for pain and reduction in size of tumours as evidenced by successful clinical trials.
PP/10/09: Work Stress among Employees Working in a Private Hospital with Reference to Christian Medical College, VelloreRekha KRojaGNagarajanPalliative Care Unit, Christian Medical College, Vellore, Tamil Nadu, India E-mail: roja.rekha76@gmail.com
Introduction: Work stress is a serious threat to the quality of working life of health-care employees and can cause hostility, aggression, absenteeism and turnover, as well as reduced productivity, interpersonal conflicts, low organizational commitment, increased absenteeism and more attrition. In addition, work stress among employees affects the quality of health-care services. The major sources of stress were inadequate pay, inequality at work, too much work, staff shortage, lack of recognition and promotion prospects, time pressure, lack of job security and lack of management support.
Objective: The objective of the study is to evaluate work stress among the employees working in a private hospital with reference to Christian Medical College, Vellore.
Method: A set of standard questions was prepared and circulated among the employees of the private hospital in Christian Medical College, Vellore. The data collected for the study were both primary and secondary in nature. The primary data was collected through personal contact with the employees of Christian Medical College and Hospital, Vellore. The secondary data was collected through books, journals, articles and websites. The tool used for analyzing is chi-square test. The analysis of the response gives the recommendations.
Recommendation: The study shows that less number of employees experiences stress which could be addressed by appointing counsellor for counselling and by focusing more in following stress management techniques, job rotation, encouragement, organizing frequent camps and recreational activities can provide better environment to control stress.
Keywords: Hospital staff, job satisfaction, management of stress, motivation, work stress
PP/10/10: Engaging Students and Youth in Community Palliative CareWarrierJyothi Jayan1Ramlabeebi2MadhavanSusheela1Volunteer, Academic Programs, Institute of Palliative Care, Pain and Palliative Care Society, Thrissur, Kerala, IndiaCoordinator, Academic Programs, Institute of Palliative Care, Pain and Palliative Care Society, Thrissur, Kerala, India E-mail: jyothijayan2003@yahoo.co.in
Background: Engaging students in Palliative Care will help to spread awareness in the community, bring about a qualitative change in the attitude of students and youth towards fellow humans and ultimately benefit the patients.
Methods: (1) Identify interested students from higher secondary schools and colleges in Thrissur District, through various social service schemes in the campus. (2) Offer structured training in Palliative care basics and communication and TOT Programs. (3) Linking them with local Primary Health Centres and palliative care units. (4) Students conducting surveys in areas where Palliative care hasn’t reached and assessing the need. (5) Involve the students in Home care services with the staff nurses who have been trained at The Institute of Palliative Care, Thrissur. (6) Monitoring also done by Institute of Palliative Care through reporting at the monthly Community nurses meetings and coordinate with program officers in the campuses.
Results: The Institute of Palliative Care has been able to educate and engage students in 5 taluks of the district by linking the local Primary Health Centres and educational institutions. Those students who have had the experience of caring for the terminally ill and bedridden, opined that, it has brought about a positive change in their approach to life. Palliative care awareness could be spread to a wider area and more patients receive regular follow up and care.
Conclusion: Students realise their duty towards the society and stand up for the rights of those who are suffering. They take active part in rendering home care and coordinating other programs hand in hand with nurses and volunteers, The students receive formal training and field work experience. This has a far reaching impact in the community based palliative care.
Keywords: Community, engage, patients, students
PP/10/12: Review of Palliative Care Services in NepalMundayDanielBasnyatReginaPoudelBishnu Dutta1RussellRuthPalliative Medicine and Health Services Research, International Nepal Fellowship Kathmandu, NepalDepartment of Medical Oncology, National Academy of Medical Sciences, Kathmandu, Nepal E-mail: daniel.munday@inf.org
Background: Nepal is a low-income country (LIC) of 28,000,000 people. As in other LIC disease demographics are shifting with increasing numbers dying from non-communicable diseases, making palliative care increasingly important. A signatory of the 2014 WHA Declaration, Nepal is committed to developing appropriate evidence based models of palliative care. As part of a needs assessment to inform palliative care development we undertook a baseline review to ascertain current provision.
Method: A questionnaire combining single answer and open-ended questions was designed to capture information on: clinical services, drug availability and education provided. Palliative Care services were identified through Nepalese Association for Palliative Care (NAPCare). A key staff member was interviewed at each institution. Analysis used MS Excel for descriptive statistics and Word for thematic analysis of free text answers.
Results: 21 institutions were identified: 13 hospitals, five hospices, two community service and one teaching institution. Eight were private, six NGO and seven government institutions. 13 provided palliative care services for cancer patients only. Eight units had palliative care beds, 61/78 (78%) of these were in Kathmandu and there were five community services. 17/20 clinical services indicated that morphine was readily available. Four institutions provided regular introductory palliative care education for a variety of health workers and NAPCare ran a yearly course on behalf of the government. Several nursing and medical colleges include palliative care on their courses but there is no specialist education.
Conclusions: There are many more palliative care services in Nepal than reported in a global review in 2013. Services were mostly in cities making the 83% of the population living in rural areas underserved. Morphine is widely available, unlike in many other LICs and palliative care education has become an important focus for palliative care providers.
Keywords: Education, Nepal, opioids, palliative care
PP/10/13: Improving Malodour Management in Advanced Cancer: A Ten-year Retrospective Study of Topical, Oral and Maintenance MetronidazolePrasoonaThotampuri ShanthiDepartment of Palliative Care, Christian Medical College, Vellore E-mail: shanthiprasoona@gmail.com
Aim: To improve malodour control using metronidazole and to explore the mechanisms underlying refractory malodour in necrotic cancers.
Methods: We studied our pattern of metronidazole use over a decade, and compared outcomes when topical, intermittent oral, and maintenance metronidazole were used. We reviewed literature to identify chemicals causing malodour.
Results: Amongst 179 patients treated for malodour, the commonest primaries were cervical (45%), and head and neck cancers (40%). Outcomes were poor during the period when only topical, or intermittent oral metronidazole was used. Topical use gradually decreased (97% vs. 55%) and the proportion of patients receiving maintenance oral metronidazole increased (0% in 2003-4 vs. 93% in 2011). Concurrently, there was reduction in documented malodour (12.5% of visits per patient in 2003-4 vs. 1.5% in 2011. p < 0.01). Recent literature, identifies dimethyl trisulphide, produced by anaerobic necrosis as the chemical that causes malodour and attracts maggot-producing flies to decaying tissues.
Conclusions: Our data supports formulary guidelines recommending maintenance metronidazole for recurrent malodour. To reduced anaerobic malodour in vulnerable settings we propose a ladder for metronidazole titration. High risk patients should start with 400 mg t.d.s. X 7 days and continue 200 mg o.d. The SNIFFF severity (Smell-Nil, Faint, Foul or Forbidding) can guide follow up dosage: 200 mg o.d. to continue for nil or faint smell; breakthrough courses of 400 mg t.d.s. X 1week for foul smell, and 2 weeks for forbidding smell. The effectiveness and limitations of maintenance metronidazole and the SNIFFF ladder should be prospectively evaluated.
PP/10/14: An Evaluation of the Impact of the Makerere Palliative Care Unit Research Network and Capacity BuildingMhoiraLeng123LucyRobinson134ElizabethNamukwaya1RebeccaCordner13Scott AMurray5LizGrant2JuliaDowning12Makerere and Mulago Palliative Care Unit, Makerere University, Kampala, UgandaGlobal Health Academy, University of Edinburgh, EdinburghCairdeas International Palliative Care Trust, Aberdeen, UKUniversity of Newcastle, New South Wales, Australia E-mail: mhoira@gmail.comPrimary Palliative Care Research Group, University of Edinburgh, Edinburgh
Background: The generation of palliative care (PC) evidence in low resource settings though supported by the WHA resolution however is often limited by research capacity. A key objective for a new academic PC unit was to encourage a research culture, supporting and initiating research nationally and internationally by capacity building through development of research networks, agendas, research workshops and training, collaborations, supervision and mentorship. We wished to evaluate the outcome of this research network's capacity building, conducted in partnership with key stakeholders.
Method: Review of internal research capacity noting projects completed, abstracts presented, publications and research qualifications attained. Evaluation of 4 research trainings held internationally; short research workshops (India, Zambia), annual research modules for BSc in PC & advanced PC research school for Africa (Uganda). Online survey followed by purposive sample of qualitative interviews included all participants covering research involvement, confidence in research process, dissemination & challenges.
Results: Academic PC unit; qualifications 5 BSc, 2 Masters, 1 Phd. 103 abstracts at national & international conferences & 11 papers published. Online survey with 56 (of 130) respondents from 9 countries. 94% working in clinical PC with 32% government & 42% NGO. 63% attended no other research training. Significant improvement in confidence (p < 0.001) after training in all aspects of research process. Participants valued supervisors’ expertise (x̄ = 3.71), quality of relationships (x̄ = 3.63) & feedback (x̄ = 3.56) though reported challenges with ethical approval (x̄ = 3.46) access to the literature (x̄ = 3.21) & internet (x̄ = 3.41). Participants noted: ‘it was very rewarding, motivating & built my confidence as an upcoming researcher’. Further evaluative data will be available through qualitative interviews of participants.
Conclusion: Results suggest the importance of research capacity building & demonstrate changes in confidence in research through training. Combining evidence based practise with clinical modelling is an important strategy within an integrated health systems approach for PC.
Keywords: Education, evaluation, research capacity
PP/10/15: Defining the Challenges in Holistic Palliative Care Provision: Opportunities for Comprehensive CareBarnardAlanDivision of Family Medicine, Faculty of Health Sciences, School of Public Health and Family Medicine, University of Cape Town, Cape Town, South Africa E-mail: abarnard@intermail.co.za
Background: It is easy to say that we must care for the patient and family holistically, but understanding and implementing that care is most important. A key to executing a comprehensive and appropriate management plan for patients with complex needs, especially in palliative care, is systematically to consider the opportunities for better care; Then to identify the challenges which impede good care and make the necessary changes to the patient management plan.
Method: This is a case study of the implementation of a practice tool in a real life clinical scenario. The application of an analysis tool and completion of an analytical grid affords a visual conceptualisation of holistic care, especially the challenges and opportunities evident.
Results: The case is presented and the value of understanding the visual depiction of holistic care is discussed.
Conclusion: The final product of the analytical process shows that explicit and visible thinking, as encouraged in the use of the clinical tool’ has the potential to be used widely.
Keywords: Holistic care, palliative care, patient management plan
PP/10/16: End-of-Life Care Issues in Rural Tribal Communities of North-West MaharashtraSinghAshita RebeccaPalliative Care Unit, Emmanuel Hospital Association, Nandurbar, Maharashtra, India E-mail: ashitasingh@live.com
Background: Very little is known about the wishes, desires, and realities of life for people with terminal illnesses in rural India. Many factors contribute to poor end of life care including poverty, illiteracy and inequitable distribution of modern medical resources. This study was undertaken at Chinchpada Christian Hospital (CCH), Nandurbar, Maharashtra among rural tribal communities to understand key wishes and desires of patients and their caregivers at the end of life.
Method: A structured interview using a descriptive approach was administered to patients with life-limiting illnesses and their families visiting CCH and those enrolled in the home-based palliative care service. Forty participants were included over a period of one month following permission by the Institutional Ethics Committee of the organization. Data was analysed using frequency, percentage and the Chi-square test where appropriate.
Results: Only 15% of patients had accurate knowledge about their diagnosis and prognosis. Less than half (45%) wanted details about their disease, and 40% were completely uninvolved in decision-making regarding their treatment. Financial constraints for treatment were acknowledged by the majority. Over 75% of patients had received futile alternative treatments; 10% had never been to a hospital. Chronic renal failure is common in this area but renal replacement therapy is unknown and impossible due to extreme poverty. None of the three HIV patients were on treatment. A small proportion had heard of mechanical ventilation (22%), dialysis (7%), and CPR (20%). Most (92%) subjects valued whole person care and 70% considered existential issues as very important. All considered relationships as highly important but sharing of fears and anxieties did not have similar value.
Conclusion: Meaningful and relevant end of life care initiatives in this rural area must allow true patient autonomy and help with avoiding futile treatment. This can be achieved through education and awareness-building among patients and family. Existing strong family bonds can optimise quality end-of-life care keeping the patient's desires at the centre of all decisions.
Keywords: Desires, end-of-life care, poverty, rural, tribal
PP/10/17: Psychosocial Aspects in Neurodegenerative Disorders: A Model for Service DeliveryThomasPriya TreesaBBhuvaneshwariWarrier GManjushaDepartment of Psychiatric Social Work, National Institute of Mental Health and Neuro Sciences, Bengaluru, Karnataka, India E-mail: priyathomasat@gmail.com
Everyone facing life-threatening illness will need some degree of supportive care in addition to treatment for their condition. In neurological disorders with potentially life threatening prognosis, the shift from cure to care is difficult to achieve. Given the irreversible nature of the illness, the multiple dimensions of care and diverse needs must to be given due importance. In the social and cultural context that is unique to India, family has a major role to play in decision making as well as direct caregiving for the patient.
The paper presents a model for psychosocial care delivery in neurodegenerative disorders. Families are partners in care and it is essential to cater to the informational, emotional and practical needs of the affected individual and family as part of the care delivery. Psychiatric Social Workers as part of the multidisciplinary team in providing care for the patient play a major role in catering to this need. Rolland's (1987) psychosocial typology of illness is presented as a feasible framework to understand and intervene with the psychosocial aspects of neurodegenerative disorders. The insights and learning points from working among patients with Motor Neuron Disease, Advanced Dementia, Advanced Parkinson's Disease who were receiving treatment from a national tertiary referral centre for Neurological disorders are discussed.
Conclusion: A conceptual framework for intervention based on Rolland's Psychosocial typology of illness is a valuable tool in service delivery with Neurodegenerative disorders. The Knowledge, skills and facilitative and challenging conditions for integration of psychosocial care into routine care will be discussed.
PP/10/18: The Impact of a Palliative Care Spiritual Intervention Program on Patients’ Well-being through a North Indian Domiciliary Care Hospice ServiceWardBrendaChaturvediAditiDCassidyDepartment of Palliative Care, Ganga Prem Hospice, Rishikesh, Uttarakhand, India E-mail: brendajward21@icloud.com
Aim and Objective of the Study: This pilot study will seek to evaluate the impact of providing spiritual care as an integral part of hospice care for patients in India, focusing on patients served by Ganga Prem Hospice (GPH) in the state of Uttarakhand.
Methodology: This study is being undertaken by a team who regularly provide home hospice care to cancer patients residing in Rishikesh and environs. This study consists of an initial patient screening, consent to engage in spiritual care (SC), and a series of subsequent SC visits for those requiring intervention. A selection of patients will also have with an integrated patient assessment in order to evaluate any change in the patient's well-being from the initial to final stage of each spiritual intervention.
The SC specialists that conduct home visits alongside the medical and nursing personnel, regularly screen patients for signs of spiritual distress and/or spiritual need. A spiritual intervention is subsequently offered to those patients that exhibit signs of spiritual distress and/or spiritual need. Those patients exhibiting signs of spiritual distress/need and agree to engage in a spiritual intervention are included in the study. Usual care continues in those patients declining to engage.
Screening Tool: The initial screening consists of 5 questions based on the Indianised version of the FICA tool. If a patient is determined to be in spiritual distress or have a spiritual need, they are a candidate for a spiritual intervention. This is offered to patients verbally, during which they are also asked for their consent to be a research subject.
Spiritual Interventions: A spiritual intervention may consist of in-depth discussion or may be practice-based, in which a request for a specific kind of spiritual observance that has become difficult for the patient to undertake is provided by GPH.
A statistical analysis will be carried out.
Results will establish the percentage of patients in spiritual need/distress and the percentages of interventions required. Results to date. Currently 25 patients have been screened. Of those, 20% exhibited spiritual distress, 12% had a need. Interventions include singing bhajans and, arranging a patient to be taken to the local temple. Evaluations on the interventions provided are yet to be carried out formally. The anticipated outcome of this study is conclusive evidence of patient benefit from spiritual care as part of their hospice care.
Keywords: Hospice care, spiritual care, spiritual distress
PP/10/19: Group Therapy as an Instrument in Facilitating Social Support for Breast Cancer Out Patients: An Exploratory StudyVaidyaMugdhaDeshpandeAruna1ThatteNandini2Department of Physiotherapy, Cipla Palliative Care and Training Centre, Pune, Maharashtra, IndiaDepartment of MSW, Cipla Palliative Care and Training Centre, Pune, Maharashtra, IndiaDepartment of Research and Training, Cipla Palliative Care and Training Centre, Pune, Maharashtra, India E-mail: nandini.thatte@gmail.com
Background: Patients of breast cancer suffer from a myriad of problems that affect their life physically and socially. Patients who are admitted to the centre interact with other patients and this interaction seems to help their social life. This does not happen with patients treated on out patient basis. The efficacy of physiotherapy in improving their mobility and activity has been documented in many studies. We examine the role of physiotherapy administered in groups on the social aspect of these patients’ lives.
Method: Patients of breast cancer opting for out patient treatment were selected for the study. A series of group physiotherapy sessions were conducted for them, over a span of two weeks. Each session was followed by a social sharing session facilitated by the social worker. The proceedings of these sharing sessions were analyzed qualitatively for factors like participation, enthusiasm, group climate, content of discussion, supportive and help seeking behavior, both inside and outside the centre.
Results and Conclusion: It was found that group exercises and sharing sessions helped in reducing social burnout, adherence to physical exercises and provided a platform to share their personal experiences and problems among themselves, thus, building a positive support system for the patients. Their interaction with other patients during the sessions, gave them the capacity to interact more meaningfully with people outside the Centre too.
Keywords: Breast cancer, group therapy, physiotherapy, social sharing, social support
PP/10/20: Learning to Be Self AwareGoswamiDinesh ChandraPalliative Care Unit, Guwahati Pain and Palliative Care Society, Guwahati, Assam, India E-mail: goswamidcg@gmail.com
Importance of self awareness is crucial to the outcome of Palliative Care. Achieving the potentials of palliative care needs exploration of self to begin with. This is followed by developing power to explore others. A narrative examines the importance in managing escalating suffering at the end of life.
Self awareness is an area of complicated human psychology and motivation. Maslow's hierarchy of needs and Johari's window are fundamental to learning Self awareness. A simple way to learn Self awareness lies in car driving principle of “Stop, Look and Go”. A good driver allows others to move along. A caregiver in palliative care leads himself as well the patient towards growth and freedom. Freedom is from suffering, which is the tenet of Palliative care irrespective of death ensues or not. Self awareness allows us to find out who we are, and what we can offer by nourishing ourselves through exposition to the narrative described. Reflective practice is the way out to learn Self awareness.
Keywords: Interpersonal care, Johari's Window, Maslow's hierarchical need, palliative care, self- awareness
PP/10/21: Palliative Care Coverage: Role of Pallium IndiaRSSheebaTraining Coordinator, Pallium India, Thiruvananthapuram, Kerala, India E-mail: education@palliumindia.org
Background: Pallium India's, Trivandrum Institute of Palliative Sciences (TIPS), WHO Collaborating Centre for Training and Policy on Access to Pain Relief, is organizing CCPPM, CCPN and CCPC courses for medical professionals. TIPS organize 4 to 5 courses per year and have been doing this since 2007. The Palliative Care coverage in India as such is minimal. One aim of Pallium India is to establish palliative care centers outside Kerala in order to spread Palliative care. This can be achieved through training of doctors and nurses from those places where there is no/scarce Palliative Care. This study would help TIPS to assess how far we have succeeded in spreading palliative care in India as well as outside India.
Objective: (1) Find out how Pallium India was helpful in spreading Palliative Care in India. (2) Find out how Pallium India was helpful in spreading Palliative Care outside India.
Methodology: TIPS started to organize training from 2007 onwards and still continuing. Doctors and nurses are classified according to the states from which they have established Palliative Care centers. The numbers of centres established by these professionals are calculated and marked in India's map in order to facilitate a better visualization. The centres outside India will be tabulated.
Out comes: The results will be published during the conference.
Keywords: Education, palliative care coverage, training
PP/10/22: Overall Survival Analysis of Patients with Brain Metastases Treated with Palliative Whole Brain Radiation Therapy in a Tertiary Cancer Centre of North Kerala: An AuditMSBijiDepartment of Palliative Medicine, Institute of Palliative Medicine, Kozhikode, Kerala, India E-mail: bijims@gmail.com
Background: Brain metastases carry an ominous prognosis regardless of primary status or treatment given. The median survival of untreated patients is about one month. Whole brain radiation therapy (WBRT) is the most widely used method of treating brain metastases, despite the fact that patients treated this way have an expected survival of only three to four months.
Aim: (1) To find out the overall survival of patients with brain metastases treated with WBRT in a Tertiary cancer centre. (2) To find out the correlation between the prognostic factors like age, sex, performance status, histology, primary site of tumour, number of brain metastases, other metastases, disease free interval and treatment (both before and after the diagnosis of brain metastases) with survival.
Method: A retrospective audit of all patients treated with WBRT between 1st Jan 2011 and 31st Dec 2015 was done from the patient case records. Apart from the demographic details, performance status, the site of primary tumour, histology, number of brain metastases, presence of other metastases, and treatment details were recorded and their correlation with survival was analysed. Overall survival was analysed using Kaplan-Meir method. Cox proportional regression modeling was used to analyse the correlation of various prognostic factors on survival.
Results: A total of 208 patient details were analysed. The mean age was 57 (range 20-87). 138 were male patients. The commonest primary site was carcinoma lung (63%), followed by carcinoma breast (21%). 65% of patients had only brain metastasis while rest had other sites of metastases also. Multiple brain metastases was found in 58% patients. While 89% of patients received Whole brain Radiation with a dose of 20Gy in 5 fractions, rest of them received 30 Gy in 10 fractions. Median overall survival was 4 months.
Conclusion: The median overall survival of patients with brain metastases treated with Whole brain Radiation in our centre was found to be 4 months. This is in concordance with the published literature.
PP/10/23: Epidural Analgesia and the Pain CyclePageNivedita DNirabhawaneVivek SGhooiRavindra BCipla Palliative Care and Training Centre, Pune, Maharashthra, India E-mail: ravindra.ghooi@gmail.com
Background: Epidural analgesia is used for the management of severe, chronic pain of cancer that is refractory to analgesics and adjuvants. During its use in palliation, it has been observed to reduce the tolerance to morphine and provide long-term analgesia way beyond the period of its use.
Methods: Seven patients with abdominal, pelvic or lower limb pain (VAS score >4, despite optimal morphine dose) were selected for epidural analgesia. A catheter was introduced in the epidural space at L3/4 and Bupivacaine 0.0625% administered at a rate of 2 ml/hr, for 6 days unless a complication arose. After the epidural was discontinued, morphine was initiated, if required, at the lowest possible dose and titrated upwards till VAS score dropped below 3.
Results: The requirement of morphine dropped dramatically immediately post procedure as expected, some patients did not require any morphine at all. The mean VAS score dropped from 8.42 to 2.14 (5 days) and 2.28 (90 days). Patients’ daily requirement of morphine dropped from 107.14 to 27.85 mg.
Conclusion: Tolerance to morphine is known to reduce following a drug holiday, but the effect is not known to persist so long. Interruption of the pain cycle appears to be the only explanation for the long-term benefit of epidural analgesia unless another mechanism is uncovered. A larger controlled trial would confirm this finding.
Keywords: Cancer pain, drug tolerance, epidural analgesia, pain cycle
PP/10/24: Sleep Hours as Predictor of Quality of Life in Cancer Pain PatientsSatijaAanchalSinghSuraj PalBhatnagarSushmaDepartment of Onco-anaesthesia and Palliative Medicine, Dr. B.R.A. Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi, India E-mail: anchal.satija@gmail.com
Background: Sleep disturbances like difficulty falling asleep, difficulty staying asleep, excessive sleepiness etc. are reported to range from 30-75% in cancer patients. The objective of the study was to determine the association between hours of sleep per day and quality of life (QOL) of cancer pain patients.
Methods: Patients visiting the pain clinic outpatient department (OPD) at Dr B.R.A. Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi were screened for this observational study. Adult patients with histological documented diagnosis of cancer related pain visiting pain clinic OPD for the first time were enrolled after providing written informed consent. Association between four domains of World Health Organisation Quality of life (WHOQOL-BREF) questionnaire and patient reported daily average hours of sleep was calculated with analyses of variance and Bonferroni correction.
Results: Patients who slept for seven to nine hours per day reported better QOL [physical health and psychological state (p < 0.005), environmental domain (p < 0.05)] than those who slept for lesser duration. Physical and psychological domains of QOL scored negative for patients sleeping ≥10 hours (p < 0.05). Patients sleeping for five to nine hours per day reported better relationships and social support that those who slept for less hours.
Conclusion: Sleep is an important predictor for determining QOL of cancer patients. Short sleep hours (i.e.≤4 hours) or long sleep hours (i.e. ≥10 hours) per day negatively affect QOL in cancer pain patients. Attention towards adequate hours of sleep per day for a patient is important for overall cancer pain management.
Keywords: Cancer, cancer pain, quality of life, sleep
PP/10/25: Deciding Right in Palliative CareSridharRepublicaJothimaniJosephPalliative Care Unit, RMD Palliative Care Trust, Chennai, Tamil Nadu, India E-mail: drjj40@gmail.com
Background: The aim of this abstract is to highlight that palliative care not only can ease the patient's life but also can give a new lease of life to patients. An estimated 19 million people need palliative care year. This case study is to explain how the right kind of palliative care and intensive care a patient can be again made to lead a near normal life. palliative care, a long neglected field in medicine has been treated as END OF LIFE CARE generally, but we would like to focus on another face of palliative care or shall we say give it’ A NEW COAT OF PAINT.’
Method: Case Study: Present Illness: On 29/2 a 77 year old gentleman with past h/o DM and Hypertension on irregular medications was brought to the emergency department with complains of headache, giddiness and numbness on the right side of the body and face since 2 days. history of blurred vision followed by loss of consciousness for a few minutes on 29/2/16. No history fever or seizures.
Course in Hospital: Patient was admitted in ward and a CT brain done which revealed normal study except for age related cerebral atrophy. On 29/2 at about 3.00pm patient had a sudden drop in GCS and was electively intubated and put on mechanical ventilation. Meanwhile routine investigations were found to be within normal limits. MRI Brain showed cerebellar infarct and bilateral thalamic infarctions on 10/3/16. Later patient was extubated with good saturation. Due to poor oro pharyngeal reflexes PEG tube was inserted on 10/3/16. On 24/3 patient became drowsy with poor GCS (e2m5v1). Patient was reintubated and connected to mechanical ventilation. On 1/4/16 tracheostomy done.
Patient discharged home on 16/4 with tracheostomy and BIPAP ventilation, inability to speak, inability to move upper and lower limbs. Patient had contacted a palliative care hoping for some end of life care.
The patient was admitted in our centre and initially his routine investigations were done and his infection was taken care of. Regular tracheostomy care and suctioning was done, meanwhile the patient was encouraged to have a positive attitude and to cooperate with the nursing staff, he was assured that we will not force him to do anything he did not want. Patient was encouraged to undergo regular chest physiotherapy and physiotherapy for his upper and lower limbs. Patient was put on BIPAP ventilation. Patients pain was taken care of with NSAIDs patient was also seen by a neurologist and a pulmonologist, and regular ABG's and chest x-rays were done. Patient responded well to the treatment and gradually the ventilator was gradually weaned off and the patient was now on room air and maintaining saturation well.
Patient was also encouraged to take orally and initially started on oral liquid diet which he soon tolerated well, followed by a soft solid diet. The peg feeding tube was not removed after consultation from a surgical gastroenterologist as it would be more dangerous for the patient at present. Patient initially started communicating with sign language and later started articulating small words. As patient was maintaining saturation well the tracheostomy was also removed after the patient was confident that he could breathe and cough well.
Results: Patient was also discharged from the centre much to the surprise of his attenders’, ambulant, communicating well and able to reasonably take care of his daily routines.
Conclusion: The aim of this case presentation is to show how that in spite of being referred to us for palliative care we were able to improve the general condition of the patient both physically and psychologically and give him a life which was denied to him. The study also teaches us the value of teamwork and how other therapists (physicians and physiotherapists) can work together in tandem to produce more tangible results. In conclusion, we as a palliative care team were faced with a big dilemma of how and who should decide right in these situations. Now we have put this same question for the honorable panelists and audience to decide.
Keywords: Cardiovascular accident, deciding right, palliative care
PP/10/26: Extension of the Palliative Care Link Nurse Programme From the National Referral Hospital to Hospitals Throughout the CountryJuliaDowning12FlorenceNalutaya1ElizabethNamukwaya1VickyOpia3ViolaEderu4RoseNgamita5JaneAmoris6JaneMwesige7MwaziBatuli1LizNabirye1LizGrant2MhoiraLeng128Makerere and Mulago Palliative Care Unit, Makerere University, Kampala, UgandaGlobal Health Academy, University of Edinburgh, Edinburgh, UKAdjumani Hospital and Peace Hospice, Adjumani, UgandaYumbe Hospital, Yumbe, UgandaNebbi General Hospital, Nebbi, UgandaTororo Hospital, Tororo, UgandaKibaale, UgandaCairdeas International Palliative Care Trust, UK E-mail: julia.downing792@btinternet.com
Background: The Link Nurse Programme is designed to increase access to palliative care (PC) provision within hospitals, through strengthening the capacity of nurses on the wards. It was developed in Mulago National Referral Hospital and an evaluation demonstrated its impact. Thus it was decided to extend the programme to other hospitals in Uganda in order to increase access to PC service provision.
Method: Eight nurses, currently undergoing leadership training in a Makerere-Edinburgh Fellowship Programme implemented a link nurse programme in their respective hospitals. in Naguru, Kibuli, Tororo, Kasese, Kibaale, Adjumani, Nebbi and Yumbe. Link nurses were identified from different wards in each hospitals and from surrounding health centres. Training was conducted using the PC toolkit and mentorship and supervision provided by the nurse fellows. An evaluation of the link nurse programme was undertaken by four of the Nurse Fellows, supported by their facilitators and mentors, as part of their leadership training and involvement in national level projects and advocacy.
Results: 149 link nurses have been trained and >500 patients have received PC from them. Link nurses have become members of the Palliative Care Association of Uganda, and thus part of an ongoing system of mentorship and supervision. A significant difference was seen in nurses’ knowledge/confidence after training (p<0.001). Provisional themes identified in the evaluation include: improved provision of PC, knowledge and attitudes and ability to train others training Ongoing challenges identified include managing complex issues and stock outs, however the link nurses are aware of their limitations and when they need to refer. The evaluation is ongoing.
Conclusion: The link nurse programme is a practical and successful model for integrating PC into generalist services. It is a model that can be used in a variety of settings, including linking hospitals and their surrounding health centres.
PP/10/27: Effect of Palliative Care on Pain and Quality of Life in Cancer PatientsJoyAswinKGunaseelanSAdinarayananDepartment of Radiation Oncology, JIPMER, Puducherry, India E-mail: aswinjoy@live.com
Background: The aim of palliative care is to improve the quality of life in chronic illness. Data is insufficient on magnitude of pain and impact on patients’ QOL in India.
Objective: To assess the level of pain and QOL among cancer patients and the effect of palliative care on pain and QOL. To identify associations of pain and QOL with clinical and socio-demographic factors.
Methodology: ancer patients attending RCC-OPD meeting inclusion criteria and registered in palliative care unit are invited to complete the Brief Pain Inventory and Functional Assessment of Cancer Therapy FACT-G questionnaire for QOL. Demographic variables, clinical data and treatment offered are recorded. Patients are assessed on follow-up until stabilization of symptoms.
Results: 201 patients are recruited presently. 132 patients made 2 or more palliative visits. Pain stabilization was possible in 106 patients (52.7%) with an average of 3 palliative visits. 91.5% of patients required morphine for pain stabilization with 69.7% presenting with stage 4 disease. Average pain score for 1st visit was 6.39 which improved to 4.66 for the 2nd visit. Average QOL scores (FACT-G) were 43.67 vs 45.77 vs 50.49 for 1st visit, 2nd visit and at pain stabilization. Significant negative correlation found between Pain and QOL at presentation. Severe Pain had a mean QOL score of 34 vs 50 for mild pain. Low income groups, Illiterate, Patients with advanced disease had lower QOL scores. Palliative Care improved Physical & Functional well-being sub-scores while Social and Emotional components were not benefitted to similar extent.
Conclusions: Palliative care is effective in reducing pain and improving QOL and requires multiple visits during the course of illness.
Most patients presented with advanced disease and were not benefitted by early palliative-care. Unmet need present for psychosocial interventions while physical symptoms were alleviated.
QOL for similar studies conducted abroad are higher which points to major lacunae in our support-system.
Keywords: Cancer pain, palliative care, quality of life
PP/10/28: Need Assessment of Children and Their Caregivers with Different Life Limiting Conditions and Planning Palliative Care as per the Disease TrajectoryTalawadekarPradnyaMAMuckaden1Children's Palliative Care, Tata Memorial Centre, Mumbai, Maharashtra, IndiaDepartment of Palliative Medicine, Tata Memorial Centre, Mumbai, Maharashtra, India E-mail: prad_mac@yahoo.com
Introduction: A variety of diseases requiring Palliative Care in Children show that there has to be a disease focussed approach since the disease trajectory is different for different conditions. Every disease has unique needs and they have to be considered before planning the care.
Objective: To assess the needs and concerns of Children and caregivers to provide quality care and help them to cope the situation by providing disease focused Palliative Care.
Materials and Methods: Dept of Palliative Medicine, Tata Memorial Centre, Mumbai is developing Palliative Care centres for children with various conditions like HIV, Cancer, Thalassemia, Neurological disorders and many others. A literature search and discussions with the respective disease experts has given us the insight of the different needs. The Focus Group Discussions and interviews are held with the caregivers and children with different conditions to assess their concerns and needs. The voices of the beneficiaries are valued to change the approach of the project and provide a quality care.
Results: Understanding the disease trajectory has helped policies and services to be better conceptualised and for implementation and empower the beneficiaries. Assessing and analysing the needs of the children has been helpful in planning better care and get a positive impact of the project.
Conclusions: (1) The needs are unique. (2) Physical, psychosocial and spiritual needs of caregivers and children vary according to disease trajectory. (3) Need assessment help the team to plan patient's multidimensional needs. (4) Different models of care may be necessary for different needs.
Keywords: Children, disease trajectories, need assessment, quality of life
PP/10/29: Education Support - Social Rehabilitation for Patients’ Children at Pallium IndiaWilfredSherinMedical Social Worker, Pallium India, Thiruvananthapuram, Kerala, India E-mail: sherinpereira.303@gmail.com
Background: “What will happen to my children?” is a common concern of many patient's and families. Then in the phase of a death or paralysis of a parent, children are forced to shoulder the immense burden of losses- of their parent, a better future, opportunity and hope. The socio-economic morbidity associated with these situations is extremely high. The hospital bills and the loss of employment lead to near destruction even the financial destruction of even middle class families in India. Children are forced to drop out from schools.
Objective: The activity was aimed at enabling children to fulfill their potential even in the phase of adversity of disease or death in the family.
Method: The clinical, as part of their social assessment, identifies children who run the risk of dropping out of school because of paucity of resources in the family. A scrutinizing committee comprised of volunteers and officials of Pallium India, screens and assesses submitted applications. Appropriate education support is then planned and provided. A proforma is used for documenting the needs as well as the overall growth and development of the children. The committee of volunteer's also supportive counseling and career guidance. An annual three days summer camp is provided for the children (”kuttikkoottam” meaning Kid's collective) which provides them not only avenues for personality development and career guidance but also allows them to have some fun.
Outcome: The support given eased the financial burden of education. The volunteers group and the informal kinship among the students created a support system for the students.
Conclusion: The education aid provided was a valuable social support for the children and their family and had a positive impact on their lives. Though difficult to measure we have the impression that in the majority of the cases the support improves the self-esteem, and confidence of the children.
Keywords: Care until the end, education support, social rehabilitation
PP/10/30: Pattern of Analgesic Use and Extent of Pain Relief in Chronic Pain Patients: Under Home Based Palliative CareThaniyathThomas AntonyFaculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia E-mail: thaniyan1@gmail.com
Background: Different groups of analgesics are available in market and a large number of patients is using these agents for the relief of pain, which is one of the most common symptom of disease manifestations, especially in chronic patients. Among these cohort of patients, the use of analgesics is long term. In this context, this study aimed to determine the pattern of analgesics use and the extent of pain relief in chronic pain patients under home based palliative care.
Methodology: A cross-sectional survey is carried out using a structured questionnaire among the patients who registered with home care services, with Vettoor Public Health Centre (PHC), Kilmanoor PHC and Adayamon PHC in Thiruvananthapuram District of Kerala State, India. The obtained data is analysed using Statistical Package for Social Sciences (SPSS) version 20.
Results: Thirty six patients (83.3% females) participated in this study. Mean (SD) age was 60.9 (7.9) years old. The majority (91.6%) suffered from malignancy. Analgesics used were NSAIDs (63.9%) and opioids (36.1%). The therapeutic effects of analgesics had insignificant relation to gender (p= 0.390), diagnosis (p= 0.765), or type of analgesic used (p = 0.324).
Conclusion: The chronic pain patients, under home based health / palliative care, more than 1/3rd are using opioid analgesics. The extent of symptom relief is not dependent on the type of analgesic used in this patient cohort.
PP/10/31: The Need for Integrated Care to Address Medical and Psychosocial Concerns among Long Stay Patients at a HIV Palliative Care CentreSarmaDivyaResearch and Document Associate, Samraksha, Bengaluru, Karnataka, India E-mail: divya.samraksha@gmail.com
Background: The advent of ART medicines has done much to ensure that HIV is a chronic manageable condition. Therefore, in HIV management, the intensity of palliative care needed is varied at different points of time, with the most intense level of care necessary when the person is acutely ill or in terminal stages. During these times, people are suffering from both physical and psychosocial issues and these needs to be addressed. However, the services available do not integrate aspects of physical and psychosocial care.
Methods: At a HIV Palliative Care centre in Karnataka, a case file review was undertaken of all the patients who had been admitted for more than 60 days in order to identify the major medical and psychosocial issues which they were facing and the type of care required.
Results: A total of 32 case files of patients who had been admitted for more than 60 days were reviewed. The most common issues were pulmonary and extrapulmonary TB, CA Cervix, Pneumonia, Herpes Zoster and Esophageal Candida. The patients were also dealing with many psychosocial issues like loss of hope, depression, worry about their health, worries about children, issues in disclosing status, need for reconciliation with estranged family members and fear of stigma and discrimination.
Conclusion: In phases of acute illness, people living with HIV are grappling with both physical and psychosocial issues. An integrated approach to care is therefore necessary to help them.
Keywords: HIV, integrated care, long term care, medical, psychosocial
PP/10/32: Accommodating Disability with Dignity - Lymphoedema Treatment in End of Life CareMarriRebeka MSVelaskarMAMuckaden1Department of Occupational Therapy, Mumbai, Maharashtra, IndiaDepartment of Palliative Care, Tata Memorial Hospital, Mumbai, Maharashtra, India E-mail: rebeka_mortha@rediffmail.com
Lymphoedema is the result of accumulation of fluid and other elements in the tissue spaces due to imbalance between interstitial fluid production and transport. Managing lymphoedema in patients with advanced disease is challenging, due to positive lymph nodes and wound. Many physical, psychological and social factors can affect the swelling and its management.
Multi-layer compression, decongestive therapy remains one of the cornerstones of lymphoedema management but in the end of life care, patients are often unable to tolerate intensive compression therapy and instead require a modified form of compression therapy that is gentle and comprises fewer layers. Most patients are told to live with it, much can be achieved to relieve pain and improve quality of life.
Minimal research has been conducted into the management of lymphoedema in advanced disease. This paper provides an overview of modified compression therapy treatment regime used, the most widely prescribed intervention currently employed for management of upper limb lymphoedema at the end of life where the standard line of decongestive therapy is not possible. The regime o f treatment not only relieves the physical, social and psychological symptoms but also enhances the quality of life at the end of life care.
Keywords: Decongestive therapy, lymphedema, quality of life
PP/10/34: Effectiveness of Initial Counseling Regarding Disease and Treatment to Parents of Children with Cancer and Assessment of Their Psycho Social ResponseNairManjushaDivision of Pediatric Oncology, Regional Cancer Centre, Thiruvananthapuram, Kerala, India E-mail: drmanjushanair@gmail.com
Objectives: To examine parent's knowledge of their child's cancer and treatment after initial counseling, and to assess their attitude and psycho-social responses.
Materials and Methods: 43 parents of pediatric cancer patients undergoing treatment in pediatric oncology division were invited to be part of this study during one of their hospital visits. Initial counseling about diagnosis and treatment was provided to all parents as is the standard practice. A time frame of 2 months from diagnosis was arbitrarily decided to allow for getting over the acute post traumatic stress period, and for completion of intensive phase of chemotherapy when complications are more frequent. Parents were provided a structured questionnaire containing simple questions in Malayalam and requested to record their responses.
Results: Parents of 36 leukemia patients, 3 NHL patients and one each brain tumour, neuroblastoma, ewings sarcoma and synovial sarcoma were studied. Majority of parents (36/43) had school level education only. 38 out of 43 parents (88%) knew the name of their child's cancer. 34/43 parents knew what type of treatment their child shall receive. 39/43 parents were aware of the approximate duration of treatment. 40/43 parents knew that their child would be subjected to painful procedures like LP/bone marrow examination etc., and 34/43 parents were aware that these procedures needed to be repeated multiple times during the course of treatment. All parents were aware of common side effects of treatment like nausea, vomiting and hair loss, but only 34/43 parents reported knowing about serious side effects like bleeding or life threatening infection. Hopeful attitude of getting cure with treatment and satisfaction with present treatment were reported by high number of parents (90%). 80% of parents reported being preoccupied with thoughts regarding their child's disease and having high levels of anxiety. 60% were worried regarding painful injections and 66% regarding painful procedures. Only 20% parents reported being worried about nausea and vomiting related to chemotherapy. As high as 60% of parents were afraid to send their child outside to play and 40% were afraid to send their child to school. Interestingly, 40% parents wanted more information regarding child's higher education, married life & fertility.
Conclusions: Child's disease related stress and anxiety persists in many parents even after acute period of adjustment to stress is over. A good amount of relevant information about cancer and its treatment can be imparted even to parents with school level education, and this may influence their psychosocial response. Parental knowledge about disease and various aspects of treatment may help in allaying disease related threat and make them more confident and co-operative towards staff. Pain related to injections and procedures is a major concern in parents. The study also reveals about unmet areas of psychological needs for which involvement of counselor as part of treating team may be beneficial.
PP/10/35: Strengthening Forward Backward Linkages between Palliative Care Centre and Other Tertiary Care Centers for Effective Management of Episodes of Acute Illness among People Living with HIVGorkhalParameshKSulekhaSarmaDivyaAnehosurAnnaraoBillalliShafiulla HYecharappaSharadaKammarKamalakshiPalliative Care Center, Samraksha, Koppal, Bengaluru, Karnataka, India E-mail: sulekha@samraksha.org
Background: HIV is now considered a chronic manageable condition, but there are still phases of acute illness during the course of life with HIV, either due to opportunistic infections of other HIV related conditions. Palliative care centers with effective linkages with tertiary care sector can support patients in managing these situations.
Methods: Samraksha is running a HIV Palliative care centre in Koppal Karnataka. The case files of all the patients who were referred to tertiary health services from the center in the last 18 months was reviewed to understand the pattern of referrals and the effectiveness of linkages.
Results: 43 patients were referred by the palliative care center for tertiary care. Referrals were made for surgeries as well as for managing difficult situations like pericardial effusion, severe rectal bleeding, to low platelet count. The referrals were made to other district hospitals, specialized hospitals like oncology centers or ophthalmology centers.
Certain processes were adopted at the palliative care centre to make the experience of care smooth for patients. The centre staff prepared the patient and family before admission to the tertiary care centre, explaining the diagnosis, cost of treatment and the different options they had. Accompanied referral was made whenever possible. There were systematic efforts at relationship building between the palliative care centre and the tertiary care centre, and this supported the referral process. It also created effective forward and backward linkages between the centre and other health services.
After discharge from the tertiary service, the palliative care centre continued follow ups to assess pain, counsel patients on adherence and provide home based nursing support as well as support from community volunteers wherever necessary.
Conclusion: Palliative care centers can complement the services provided by tertiary care sector in managing situations of acute illness among people living with HIV
Keywords: HIV, referral linkages palliative care, tertiary care
PP/10/36: Impact of an Educational Program on Parental1 Knowledge of Cerebral PalsyKBSakthi PrasadVolunteer, Department of Palliative Care, Alpha Palliative Care, Alappuzha, Kerala, India E-mail: Sakthiprasad03@gmail.com
Cerebral palsy is a term used to describe a group of non-progressive disorders that manifest as abnormalities of motion and posture. These disorders result from a central nervous system (CNS) injury sustained in the early period of brain development, usually defined as the first three to five years of life.
Cerebral palsy cannot be cured, but “early rehabilitation” can help achieve functional abilities that facilitate independence and improve quality of life. But many parents have lack of knowledge or awareness in treating children is the major problem in disability.
Aim: To determine the parents’ knowledge of their child's cerebral palsy and also evaluate the impact of educational intervention on it.
Setting: Alpha palliative care Hospice.
Participants: Patients registered in Alpha palliative care Hospice Alappuzha and north paravoor in 2015.
Outcome Measure: Gross Motor Function Measure (GMFM).
Results: A total of 38 cerebral palsy patients have been registered. The parents of cerebral palsy were interviewed after the interview, each parent was administered a structured educational program (educational class, treatment technique, booklet for treatment technique) and continued once in a week up to three months. The pre and post intervention responses were compared using Chi-square test.
Conclusion: Parental knowledge of cerebral palsy is highly effective. The continued educational program and treatment develops child's Gross Motor Function.
PP/10/38: Bereavement and Social Response: Need for an Alternative SystemSharmaMohita ChaturvediDepartment of Sociology, Kanoria PG Mahila Mahavidhalya, Jaipur, Rajasthan, India E-mail: mohitachaturvedi@gmail.com
A full realization of the social nature of behavior requires that one clearly distinguishes between any biological condition and the social behavior related to it. The manner in which the individual responds to a biological condition largely stems from the label he places on the condition thus, responding to the symbols. Dying is a form of behavior which has social consequences for many others, consequences related to the type of definition placed upon the deceased by the living. Thus, grief becomes a normal and healthy response to loss. Family as a social unit also bears the sorrows of death of a family member which results in multiple forms and levels of grief depending upon the tolerance and reactions of the family members. It is necessary to mention here that family and society being social institutions are dynamic in nature, the constant transformation leads to a shift in the patterns of behavior. Indian society being no exception has also undergone change resulting in the fading away of traditional support system. The need for professional help is now being realized which was earlier never thought of in reference to Indian society. The specialized care system has to work in order to ensure and reduce the possibility of further loss of life to an already grieving family. However, formal system alone cannot contribute to the coping process thus, requires a parallel and interrelated and interdependent care systems. Community participation could help in this transition and also generate the awareness about the existence of formal support system and promote its acceptance.
Keywords: Bereavement, death, family and formal care system, grief
PP/10/39: End of Life Physical Problems of PatientsNKNikhilNairKirthi SSSanthaPost Graduate Department of Commerce and Research Centre, St. Peter's College, Ernakulam, Kerala, India E-mail: nknikhilnair@gmail.com
Background: India, with a population of over a billion people, is a country of varying social, cultural and geographic characteristics. There are real problems in meeting the health care needs of such a large population, particularly, the poor in rural areas. Managing their end of life issues would be a difficult task, especially in the case of chronic, debilitating illness like chronic obstructive pulmonary disease. The available data show that patients are still receiving inadequate end-of-life care. Palliative Care represents an important resource in the completion of good medical care which can help to take the best care of patients and their families. The availability of palliative care is very limited in much of the world.
Aim: The current study has been undertaken to know the End of Life Physical Problems of Patients in Chottanikkara Panchayat, Kerala.
Materials and Methods: For the purpose of study, 50 respondents were selected as samples by adopting convenience sampling method. Analysis was done via statistical software 17.0. using statistical tool, viz. One Way ANOVA (Post Hoc Test Tukey HSD).
Results: The study revealed that most of the patients were suffering from the problems of old age and disability. There was no significant difference in the physical problem, viz. bed sore, Agitation, Dehydration, Constipation, Cachexia, Loss of function, Dyspnea (except cancer patients and patients suffering from Problems of Old Age and Disability) suffered by the patients suffering from different types of diseases before one year to last 2 weeks of their death. There was no significant difference in the physical problem- Nausea suffered by the Cancer patients and patients with Spinal injuries, Dyspnea suffered by the cancer patients and patients suffering from Problems of Old Age and Disability, Vomiting suffered by the Cancer patients and patients with Chronic Liver Disease before one year to last two weeks of their death. There was a significant difference in the physical problem- Nausea’ suffered by the cancer patients and patients suffering from Problems of old age and Disability and Chronic Kidney Disease, Vomiting suffered by cancer patients and patients suffering from Problems of Old Age and Disability Chronic Kidney Disease, before one year to last 2 weeks of their death.
Conclusion: There was a significant difference in the physical problem- Nausea’ suffered by the cancer patients when compared to patients suffering from Problems of old age and Disability and Chronic Kidney Disease and Vomiting suffered by cancer patients and patients suffering from Problems of Old Age and Disability Chronic Kidney Disease, before one year to last 2 weeks of their death.
Keywords: Analysis of variance, chronic kidney disease, dyspnea, nausea, palliative care
PP/10/40: Spotlight on Spinal Cord InjuryTGajendranDepartment of Physiotherapy, SAHAI Spinal Injuries Rehabilitation Centre, Coimbatore, Tamil Nadu, India E-mail: gaja.ran@gmail.com
Background: To analyse the aetiology, levels of injury and achieved outcome of spinal cord injury at our rehabilitation centre.
Study Design: Retrospective review.
Results: Of the 285 consecutive spinal cord injured persons treated in our Centre 206 were complete, 79 were incomplete of which 52 were quadriplegics and 233 paraplegics. Causes of injury- fall from heights constituted 60% of patients, road traffic accidents 31% and non- traumatic causes 9%. Post rehabilitation status 8% were gainfully employed, 56% mobile but unemployed and 36% partially mobile or bedridden.
Conclusion: Fall from heights and motor vehicle accidents were found to be the major causes of traumatic SCI. Preventive measures should be the main focus for this group in order to reduce the frequency of SCI. 56% continue to do functional/therapeutic walking with calipers, but not employed or earning. Social responsibility should be extended to the differently abled to enable the physically challenged to live with dignity.
PP/10/41: Will Health Care Professionals Consider Advance Directives for Themselves in the Event of a Terminal Disease – A Cross Sectional Study in an Academic InstitutionNairShobaSampathArchanaTareySubhashMathewsRickyDanielSudhaDepartment of Palliative Medicine, St. John's Medical College, Bengaluru, Karnataka, India E-mail: nair.shoba@gmail.com
Background: Advance directives are used to provide optimum health care as per the patient's wish, which is practiced more in other countries than in India. Health care professionals need to be clear on their own advance directives in case of an incurable terminal disease.
Objective: Primary - To assess health care professional's willingness and the depth to which they would to have an advance directive for themselves. Secondary - To assess the influence of experience, age, gender and profession in the health professional's decision making regarding advance directives.
Methods: Design - Cross-sectional study. Population - Doctors and nurses in a teaching hospital Ethical Considerations - Being followed by submitting to IERB. Data Collection - Self administered questionnaire. Setting and Location - Teaching tertiary care hospital in South India. Sample Size - was calculated estimating that 10% of St. John's population will be aware of advance directives compared to the population proportion of 5%, with a power of 80, α error of 5, and an expected 2 sided result. The sample size estimated was 185. Analysis - One sample t test will be used to describe the percentage of health professionals who would want an advance directive and a regression analysis to correlate factors like experience, field of work etc that would influence their decision on advance directives.
Results: This study is ongoing and the results will be presented at the conference
Keywords: Advance directive, awareness, health care professionals
PP/10/42: Advocating for Palliative Care in Efforts to Promote Universal Health Coverage and Essential Medicines PoliciesKumarAbhishekDepartment of Pediatric Palliative Care, Cankids, New Delhi, India E-mail: doctorppcp@cankidsindia.org
Palliative care services need to be provided in accordance with the principles of universal health coverage. All people, without discrimination, should have access to nationally determined sets of basic health promotion, preventive, curative, rehabilitative and palliative health services and essential, safe, affordable, effective and good-quality medicines and diagnostics.
Worldwide, provision of palliative care has to overcome significant barriers: health policies in many countries do not adequately meet the needs for palliative care; research and training are often non-existent or limited; and access to opioid analgesics is difficult to ensure. Other barriers include a lack of awareness of the great need for palliative care; insufficient or unimplemented government policies for improving the provision of palliative care; a lack of knowledge of palliative care among healthcare workers; limited availability and accessibility of opioid analgesics (especially in oral form) and other essential palliative care medications in many countries; misconceptions about palliative care; and financial and health system constraints. Social and cultural barriers (such as beliefs about death and dying) and the difficulty in ensuring ethical decision processes in life-threatening conditions also have an important impact on access to palliative care.
The need for palliative care services will continue to grow, owing in part to the rising prevalence of noncommunicable diseases and the ageing of populations everywhere. For non-communicable diseases, the need could be reduced through their early detection and timely management to prevent complications. Through strategic advocacy planning with our national and network partners to ensure that palliative care services, both institutional and home based, are included under universal coverage, and it is promoted as a basic health platform advocating for palliative care is required. Thus, through this topic I will be highlighting all the important aspects of advocacy work being done by me in India.
Keywords: Advocacy, essential medicine, palliative care
PP/10/43: A Study on Psychological Distress among Gynaecological Cancer Patients on Diagnosis Using the Distress ThermometerCJothimaniPrabha SLakshmiSKarthigaBSivanesanBalasubramaniLathaDepartment of Gynecologic Oncology, VNCC, GKNM Hospital, Coimbatore, Tamil Nadu, India E-mail: jothimani.c.t@gmail.com
Introduction: Patients diagnosed with cancer experience a high level of psychological distress. Psychological distress can be defined as an unpleasant emotional experience which may interfere with the ability to cope effectively with cancer.
Aim: The aim of the study was to evaluate the level of distress among gynaecological cancer patients on diagnosis, using the National Comprehensive Cancer Network's (NCCN) Distress Thermometer (DT).
Materials and Methods: Patients who attend Gynaec oncology outpatient following their diagnosis of cancer were administered the Distress Thermometer, a single item rapid screening tool for distress. About 30 patients were interviewed for the study. The distress Thermometer is a visual analog scale on which participants rate their level of distress from 0 to 10. Using the Distress Thermometer, we could also assess the root cause of distress in patients.
Results and Analysis: A score of 5 and above was considered a sign of distress. Our mean distress score was 6.7. When we looked at practical problems causing distress, transportation scored the highest at 40%, with insurance/finances coming a close second at 36%. Family problems, were not a cause of distress in our group of patients. The main cause of distress for patients immediately after a diagnosis of cancer were emotional problems. Fear scored the highest at 73%, with sadness and worry at 66% and 63% respectively. Amongst physical problems, inability to sleep, scored highest at 53.3%.
Conclusion: Our study shows that the majority of the patients are in high distress immediately after a diagnosis of cancer. Most problems expressed were emotional and a major proportion of patients present with inability to sleep. It is therefore important for cancer patients to have acess to counselling services to help deal with a diagnosis of cancer and cope with treatment. Distress Thermometer administered during and after completion of treatment will help in measuring trends in patient distress.
Keywords: Counseling, distress, gynec oncology
PP/10/45: HIV Specific Issues to Be Addressed in Postbereavement Support Visits to Family MembersKSulekhaKattiPrabhu NKammarKamalakshiSarmaDivyaSamraksha, Koppal, Bengaluru, Karnataka, India E-mail: sulekha@samraksha.org
Background: Family members of people living with HIV face many emotional as well as social issues some of which are specific to HIV.
Methods: Samraksha runs a HIV Palliative Care Centre in North Karnataka. The centre initiated the practice of post bereavement family support visits to help families cope with their situation better. Consent was taken from the families before the visit. Over a period of 24 months, there were 74 deaths at the centre and 66 families gave consent for follow up visits. A casework approach was used to assess the family situation and help them during the visits.
Results: The follow up visits was able to improve coping of families in multiple ways. It helped in linkages to social supports including child sponsorship and legal support for claiming of property. It also helped in providing emotional support to cope with the loss.
Additionally, in almost 50% of the cases certain issues specific to HIV could also be addressed – stigma and discrimination, accidental disclosure of HIV status following the death and coping with the outcomes of this disclosure, planning for disclosure to family members, especially children, emotional support for HIV testing for partners and children. Intensive counseling was needed to support the family members in these issues.
Conclusion: There are some specific HIV related issues which need to be addressed during supportive visits to family members after bereavement. Intensive counseling is necessary to address these issues.
Keywords: Bereavement support, family support, HIV, holistic care
PP/11/02: Quality of Life in Breast Cancer Patients and Its Association with DepressionPurkayasthaDebaswetaDepartment of Oncology and Palliative Care, Amrita Institute of Medical Sciences, Kochi, Kerala, India E-mail: debasweta@gmail.com
Background: Quality of life (QoL) has become one of the main outcome measures in cancer treatment. QoL is a multi-dimensional measure of psychological, physical, role, cognitive and social well-being. Breast cancer affects all the domains of QoL. Depression has a detrimental effect on all aspects of QoL in cancer patients and is associated with poorer medical adherence. Early palliative care improves the quality of life in these patients. We aimed to study the QoL in breast cancer patients and its association with depression.
Method: This cross-sectional observational study enrolled 270 patients diagnosed with breast cancer (>18 years) and undergoing active treatment in a tertiary care centre in Kerala state of India. QoL and its domains were measured with WHOQOL Bref. Depression was assessed using the Patient Health Questionnaire 9 (PHQ 9) and ICD 10 Research guidelines. The numerical variables were expressed as Mean ± SD and categorical variables are expressed as frequency. To obtain the mean comparison of different domain scores with depression, Independent Two Sample t test was applied. To obtain the association between QoL and Depression, Chi square test was applied. P value of ≤0.05 was considered statistically significant.
Results: The average age of women in research was 53.56 years. Twenty-two patients reported their overall quality of life was “poor” and 34 patients reported to be dissatisfied with their health. Of the 270 subjects, 21.5% had depression. Patients with depression experienced overall a poor QoL. There was an association between depression and domains of QoL. Patients with depression had lower scores in all domains when compared to those without depression.
Conclusion: Breast cancer patients have a poor overall QoL and depression may significantly impair the quality of life. Recognising and addressing depression in breast cancer can contribute towards improvement in quality of life and better outcome of palliative care.
Keywords: Breast cancer, depression, quality of life
PP/11/04: Home Based Lymphedema CareMattamAnneWarrierSreedeviShajiDanyPalliative Care Unit, Pallium India, Thiruvananthapuram, Kerala, India E-mail: annemattam@palliumindia.org
Objectives: To study the feasibility of providing lymphoedema care at home by involving caregivers. To assess the impact training caregivers and community volunteers has on improving patients’ quality of life and functional independence.
Background: Lymphoedema is swelling secondary to lymph accumulation in interstitial tissues and can occur in any cancer affecting lymph node drainage.
Cancer survivors with lymphoedema experience more psychological distress, disability and a poorer quality of life. Furthermore, if lymphoedema is not diagnosed and managed early, the chances of it becoming increasingly severe is much greater. There is therefore a need for raised awareness regarding the importance of its early detection and management.
Pallium India provides home care services within 14 panchayats in the Trivandrum District in collaboration with local volunteers. This project focuses upon lymphoedema patients from within the same locality. The study includes 34 patients who registered with our services between November 2014 and June 2016. Those who died or dropped out were excluded.
Methodology: Initially a needs assessment study of the community was completed by the lymphoedema team (consisting of a doctor, nurse and social worker). The team provided training to the caregivers regarding lymphoedema management and followed up patients at home for a 3 month period. Improvements in patients lymphoedema was monitored by taking arm measurements at the first visit and then at intervals of 2 weeks thereafter. The team also directly supervised the care provided and provided training to community volunteers to assist in monitoring. Patient and caregiver satisfaction was assessed using a questionnaire.
Out comes: Improved lymphoedema care. Improved functional independence. Increased awareness about lymphoedema care being provided at home. Increased community awareness.
Long Term Outcomes: Increased awareness and involvement of the community can help patients and their families cope with lymphoedema and its physical and psychosocial consequences.
Observations: (1) 1 patient experienced marked improvement of their lymphoedema. The greatest response was seen in those whose lymphoedema was detected early. (2) patients were unable to practice lymphoedema care at home due to a of lack of caregivers and were noted to have a deterioration in their condition. In 21 patients no significant changes in their condition was observed. Those suffering from lymphoedema require dedicated attention and follow up. Empowering home care teams, patients, caregivers and community volunteers is essential.
Background Reading:
Lymphoedema, estimating the size of the problem (Williams AF, Franks P.J, Moffat C.J- Palliative Medicine 2005, June).
Incidence and Prevalence of Lymphoedema - A literature review (Logan V, J. clinical Nurs-1995).
Managing chronic edema - A collaborative community approach (Lewis M, Morgan K- British Journal of Community Nursing-2008).
Lymphoedema care of breast cancer patients in a breast cancer clinic- A survey of knowledge and health practice (Lee Y.M, Mak S.S, Tse S.M, Chan S.J- Support care cancer, 2001 Nov.)
Lympohedema- Health Professional version - NIH- National Cancer Institute.
Keywords: Care giver, community awareness, home based care, lymphoedema
PP/11/05: Role of Neuro Linguistic Programming in Palliative CareRVijayalakshmiKAravamoothamTiruvadananMallikaMuthukumaranSubathraMathewAsokePalliative Care Unit, Lakshmi Pain and Palliative Care Trust, Chennai, Tamil Nadu, India E-mail: lakshmipaincare@gmail.com
Aim: Eliminating fears, guilt, anxiety and phobias and then bring about acceptance and forgiveness by using specific NLP Techniques in patients with palliative care needs.
What is NLP?: N (Neuro) - Brain and nervous system and how they organise our experiences. L (Linguistic) Language - verbal and nonverbal and how they impact our experiences. P (Programming) - The unconscious programmes that are run by us in our minds… NLP is a unique model which teaches people how to learn, motivate themselves, and change their behaviour to achieve excellence in any endeavour.
How to Create a Change?: By identifying the present state, desired state and the appropriate resources (internal states like physiology, emotions, feelings and sensations, skills and information) required to change from the present state to the desired state and eliminating any interference by using these resources.
How to Identify?: By using the ‘Meta Model’ – a set of explicit, specific questions to identify commonly occurring language patterns which actually hamper good communication; shows how their minds can be tackled to open up clearer and effective communication.
Method: After building a rapport with patients, we use the Dave Elman Induction or JPMR relaxation therapy to help them relax physically and mentally. We then programme their subconscious minds using techniques such as sub modalities, reframing for change, forgiveness affirmations, eliminating fears and phobias, building confidence etc., according to patients’ needs to make them comfortable.
Conclusion: By implementing these techniques it is possible to help them overcome their fear, anxiety, anger, to reduce suffering and improve quality of life.
Keywords: Communication, Neurolinguistic program, quality of life
PP/11/06: Why Some Patients Are Oral Morphine Noncompliant? (A Study of 100 Patients on Oral Morphine)MohanRavinderHead Knowledge, Education, Training and Research, CanSupport, New Delhi, India E-mail: ravindermohan@cansupport.org
Background: Oral morphine is Gold Standard in management of moderate to severe cancer pain. Non compliance to oral morphine causes lot of suffering and adversely affects the quality of life of patients and their caregivers. Non Compliance to Oral Morphine is a matter of great concern. This study aims at finding reasons of morphine non compliance among patients on oral morphine and how to address these reasons of noncompliance.
Methods: One Hundred patients on oral morphine were included in this study. In the patient with non compliance to oral morphine a questionnaire was used by the health care provider to understand the reason of non compliance to oral morphine. If the reason for the non compliance is not listed in the questionnaire the health care provider added that reason in the list of reasons of non compliance.
Results: The foremost reason for morphine noncompliance found in this study was “family physician or some other doctor advised to stop oral morphine.”
Conclusion: The doctors at large are not aware about the role of oral morphine in cancer pain management and need to educate doctors on this issue is real and urgent.
Keywords: Awareness, education, opioid, non complaince
PP/11/07: The Importance Volunteers Presence in the Total Palliative Care StructureDBhoopathy1ParameswarJannet2Volunteer and Counselor, Bengaluru, Karnataka, IndiaSocial Welfare Officer, Department of Palliative Care, Kidwai Memorial Institute of Oncology, Bengaluru, Karnataka, India E-mail: naidums2003@gmail.com
Aim: To evolve an organized and structured service for the volunteers as a part of total care structure in the hospitals. The total care structure module should involve people (NGO's, Social workers, Philanthropists etc.) from all walks of life to ease the pain and suffering of the patients.
Background: For a cancer patient, medical treatment is the priority. Various schemes under govt schemes (Jyothi Sanjeevini, Vajpayee Arogya Bhagya Yojane, Yeshesvini, Chief Minister fund, SC-ST schemes. ESIC.etc.) provides free medical aid to the patients.
23 medical social welfare officers (SWO) of KMI have to assist, guide and counsel around I,40,000 patients who avail the free medical aid. Considering the huge turnover of the patients, the heavy load of work, long working hours and laxity of time, invites the assistance of volunteers’ service which is complementary. One psychologist is not sufficient to address the psychological, social, cultural, spiritual issues of the all the patients.
Few care teams (doctor, nurses, swo, volunteers) functions in pediatric, palliative wards and in Dharamshala dormitory. Volunteers, philanthropists, nursing, PG students, psychology students from colleges and schools and, NGOs, humanists visit the patients regularly. But, it is not covering the all units of the hospital patients. It is only tip on the iceberg. Hence there is a need to organize and expand the permanent volunteer service in a systematic and organized manner.
Materials and Methods: 12 medico social welfare officers (SWO), 10 volunteers and 10 caretakers were individually interviewed with an oral questionnaire. SWOs were asked about their workload, job satisfaction and the existing facilities and need for voluntary assistance. The volunteers and care takers were questioned about the need of volunteer service and their work facility and satisfaction.
Results: (1) With regard to SWO: (i) 75% need training and support in accounting and data entry. (ii) 60% need support of clerks, helpers and volunteers. (iii) 80% wants one single care structure module in the hospital. (2) About patients and care taker: (i) 90% preferred the presence of volunteers. (ii) 80% are happy with the emotional and social support given by the volunteers. (iii) 70% of them agreed that the volunteers support reduce their overall stress. (3) About volunteers: (i) 75% volunteers felt their service is not fully utilized in hospital. (ii) 60% prefer clinical training and involvement in projects, awareness and education programs. (iii) 80% felt their service is not evaluated nor documented scientifically.
Conclusion: There is a dire need for structured volunteer service. Each hospital should have permanent volunteer service cell and clinical cell with trained volunteers in various alternative therapies. Their work should be guided, supervised, assessed and documented, statistically by the hospital staff.
In KMIO Dharamsala (Dormitory), all 300 in patients are satisfied with the service module provided to them. This successful integrated module was created by ex-director Dr. Bhargava, assisted by Dharamsala Committee includes Director, volunteers and donors. It has got 24 hours emergency room and rehabilitation center engaging caretakers and cancer survivors. Regularly patients are entertained with cultural programs.
The one SWO therein, is assisted by 12 helpers. The in-patients are happy with the regular visits of the committee members. All patients’ feel very homely under the Dharmasala care structure. The Social Welfare Dept., of the govt. and all the hospital committees can build on this particular model to prepare a central and comprehensive care structure to the patients involving the trained volunteers.
Keywords: Care structure, Social Welfare Officers, volunteer service
PP/11/08: Scrambler Therapy Manages Cancer Pain and Improves Quality of LifeKashyapKomalSinghVishwajeet1BhatnagarSushmaDepartment of Onco-anesthesia and Palliative Medicine, IRCH, AIIMS, New Delhi, IndiaDepartment of Biostatistics, AIIMS, New Delhi, India E-mail: komalkashyap009@gmail.com
Background: More effective treatment is needed for cancer pain. Preliminary data support the use of scrambler therapy, a device which treats pain via non-invasive cutaneous electro stimulation, for the treatment of cancer pain. The current abstract reports data from a pilot trial, performed to investigate the effect of scrambler therapy on quality of life in patients with chronic cancer pain.
Methods: Prospective observational study conducted on patients with chronic pain due to malignancy which is not responding to oral analgesics.
A total of 20 patients were included in the study (10 males, 10 females) with a VAS score of >4 on oral analgesics. Patients aged 18-70 years with a life expectancy of >3 months having bony, neuropathic, or mixed type of pain were included in the study. A total of 12 sessions of scrambler therapy were planned, 10 sessions on consecutive days and one session each on two follow up visits after one week each. Each session lasted 40 minutes. Pain relief and quality of life according to WHOQOL were recorded as primary outcome variables.
Results: All patients had good pain relief and improvement in all 4 domains of quality of life i.e. physical, psychological, social and environmental health (p < 0.01) after the therapy.
Conclusion: Scrambler therapy offers a promising role in the pain physician's armamentarium as an adjunct to pharmacological therapy for treatment of chronic drug resistant cancer pain; it may bring down analgesic drug requirements significantly and improve quality of life in cancer patients.
Keywords: Chronic pain, scrambler therapy, visual analog scale, World Health Organisation Quality of life
PP/11/09: Challenges in Setting Up a Care Plan for the End of LifeLouisMaria SoniaSimhaNageshJohnsonJeremyKarunashraya, Bangalore Hospice Trust, Bengaluru, Karnataka, India E-mail: jeremy.johnson@karunashraya.org
The IAPC has long been an advocate for developing a Policy for End of Life Care (EOLC) and together with the ISCCM has suggested guidelines regarding an Integrated Care Plan for the dying.
More recently members from several palliative care units around India came together and agreed to participate in adopting the ten principles espoused by the International Collaborative for Best Care of the Dying Person (ICBCDP) and form “Project India”. As an independent Hospice, Karunashraya, in Bangalore, was tasked with piloting the initial implementation.
The first step was to develop clear, user-friendly documentation that encompassed the various key elements. These resolved into three sections: (1) Multidisciplinary team recognition that a patient was dying, and initial assessment of the patient's individual needs (medical, nursing, social, emotional and spiritual), (2) Addressing ongoing problems, and providing support for the family. The documentation here acted as an “aide memoire” in identifying concerns, in addition to acting as a daily record of evolving changes. It helped focus on the nursing and social issues and to identify symptoms requiring anticipatory prescribing by the medical team. (3) Care after death.
Learning Points: (a) The need for extensive feedback from the nurses, medical team and counsellors in achieving a workable, pragmatic final draft with which the whole team felt happy and confident. (b) The considerable time needed for ongoing education, discussion and monitoring. (c) Need for excellent communication both verbal and written (leaflets produced in different local languages). (d) Establishment of clear written policies within the organisation, particularly regarding Care after Death (certification, handling the body, handing over to relatives, written information regarding registration, facilities available and bereavement support).
Keywords: End of life care plan, project India, staff education
PP/11/10: Based on the Prevalence of Noncommunicable Diseases, What Is the Projected Need for Palliative Care in Nepal?SwarbrickEleanorMundayDaniel1PietroniMark2Medical Student, University of Bristol, UkConsultant, Palliative Medicine, International Nepal Fellowship, Kathmandu, Nepal E-mail: e.swarbrick.2013@my.bristol.ac.ukDirector of Public Health, South Gloucestershire, UK
Background: Despite a high burden of non-communicable diseases (NCD), both data availability and provision of palliative care in Nepal are limited. As part of a nationwide needs assessment and to inform palliative care development, a modelling exercise was conducted with the aim of estimating the scale of the current need for palliative care.
Method: Based on the recent Global Atlas of Palliative Care's method, quantified estimates of the minimum projected need were generated by multiplying World Health Organization population-level estimates of mortality by cause for commonly occurring chronic conditions in Nepal and prevalence of pain by disease. Projections were then broken down based on location, disease and age. A literature review was also conducted to provide context, to enable an assessment of urban versus rural need and evaluate palliative care provision.
Results: The highest burden for palliative care in adults was cardiovascular disease (CVD), whose prevalence is particularly high in urban areas and is likely to be rising. Chronic obstructive pulmonary disease and cancer together with CVD made up 75% of the need in adults. 6% of the need for palliative care is in children with the commonest conditions being congenital abnormalities and neonatal conditions. 63% of the need for palliative care is in rural areas.
Conclusion: This research provides a crude estimate of the need for palliative care in Nepal. Comparing need with provision from a recent service review suggests that current provision does not adequately meet needs. Limitations of this study include the uncertain reliability of the data used and questions about the transferability of the Global Atlas’ Palliative Care method to the context of Nepal. Surveys of incidence and mortality from NCDs and illnesses requiring palliative care are needed to provide more reliable estimates of the need for palliative care.
Keywords: Nepal, non-communicable diseases
PP/11/11: Utility of Charcoal in Palliative CareSVatsalaSeshacharPrabhaAnandJulietDepartment of Palliative Medicine, Kidwai Memorial Institute of Oncology, Bengaluru, Karnataka, India E-mail: madhavtr71@gmail.com
Charcoal is an inert substance and a good adsorbent. When taken orally, it relieves gas, indigestion, nausea, diarrhoea, drug overdose and several other conditions. Adsorption is a surface phenomenon. By powdering charcoal, its surface area and absorptive capacity are increased. Hence nanoparticles of carbon adsorb better. In Japan, a commercial product of nanocarbon; AST-120, is administered to patients with chronic kidney disease, which helps in postponing the need for dialysis appreciably, as the carbon adsorbs indole in the gastrointestinal (GI) tract, which is the precursor of indoxyl sulphate, a uraemic toxin. Homeopathy practitioners use carbo vegetabilis i.e. vegetable charcoal, for various conditions. It is nicknamed ‘orpine reviver, as it is capable of reviving an about to die patient. In 18th and early 19th centuries, mystics in their trance advocated the use of charcoal, both orally and also for local application. Ellen G. White (1827-1915), the prophetess who founded the Seventh-day Adventist Church, during her ‘visions’ recommended pulverised charcoal both internally and as poultice as a remedy for various ailments. Dr. John Harvey Kellogg M.D. (1852-1943), an American medical doctor, the inventor of corn flakes, prepared charcoal tablets with honey. These tablets were referred to by the ‘sleeping prophet’, Edgar Cayce (1877-1945), during his ‘readings’. Edgar Cayce, was a Christian mystic who answered questions in various fields including healing, while in trance.
At the Kidwai Memorial Institute of Oncology, Bengaluru, we use charcoal capsules to relieve nausea, diarrhoea or any other discomfort in the GI tract, charcoal poultices for miraculous relief from pain, and charcoal powder to remove malodour the cancerous wounds with impressive outcomes.
PP/11/12: Adapting the Supportive and Palliative Care Indicator Tool (SPICT™) for Use in Rural NepalMundayDanielRussellRuthBKManjuMurrayScott1BoydKirsty1Department of Palliative Medicine, International Nepal Fellowship, Kathmandu, NepalDepartment of Palliative Medicine, Primary Palliative Care Research Group, University of Edinburgh, Edinburgh, UK E-mail: daniel.munday@inf.org
Background: Identifying patients who could benefit from a holistic needs assessment and palliative care approach is vital for providing palliative care and for case finding in needs assessment research. SPICT™, a simple tool designed for patient identification, is being adapted in various countries. We report how we are developing SPICT™ for use in rural Nepal.
Method: The UK version of SPICT™ (www.spict.org.uk) was modified by experienced palliative care clinicians in Nepal. This was then used in a survey of palliative care in a rural 166 bed general hospital. Patients with advanced illness were assessed using “NepalSPICT™” then clinically by an experienced palliative care clinician. The two assessments were compared and discussed by the team to ascertain whether further modifications were needed to improve NepalSPICT™ sensitivity and specificity.
Results: Initial modifications included adding multidrug resistant TB and replacing “Needing long term oxygen therapy” with “O2 saturation persistently <90%.” 66 patients were identified with Non Communicable Diseases and assessed using NepalSPICT™. 23 were identified as likely to have palliative care needs. Further modifications to NepalSPICT™ have been made. For example a performance scale was devised to replace the item “Performance status is poor or deteriorating (the person is in bed or a chair for 50% or more of the day)” – as the concept of being in bed or a chair for 50% of the day is not culturally appropriate.
Conclusion: SPICT™ is an adaptable tool which is easy to use and appears to be appropriate for use in rural Nepal by nurses and doctors to identify people for generalist palliative care. We plan further evaluation and modification as part of a community survey. This work could also be useful in developing SPICT™ for use in other low-income countries. We welcome collaborators to do this.
Keywords: Development research, indicator tools, palliative care
PP/11/13: A Palliative Care Curriculum Toolkit: A Practical Guide to Integrating Palliative Care into Health Professional EducationKSnellSMurray1LGrant2ABarnard3JDowning45MLeng246University of Zambia, Lusaka, ZambiaPrimary Palliative Care Research Group, Centre for Population Health Sciences, University of Edinburgh, EdinburghGlobal Health Academy, University of Edinburgh, EdinburghUniversity of Cape Town, Cape Town, South AfricaMakerere and Mulago Palliative Care Unit, Makerere University, Kampala, UgandaInternational Children's Palliative Care Network E-mail: mhoira@gmail.comCairdeas International Palliative Care Trust, Aberdeen, UK
Background: The integration of palliative care (PC) in education programmes is a crucial component of health system strengthening and is emphasised in the WHA PC resolution (2014). Health care curriculums are congested and newer designs focus on competencies and outcomes rather than stand-alone courses. In India, efforts are being made to progress curriculum integration but it has been very slow. In response to requests from academic colleagues and as part of a wider health systems strengthening approach a Toolkit was developed to support integrating core PC competencies into curriculum planning which builds on existing PC competency frameworks.
Method: An expert group from 4 academic settings and 3 global health and PC organisations convened to review existing competency frameworks, draft an outline and develop a Toolkit. The aim was to support; comprehensive review of PC in an established curriculum; integration of PC components into a curriculum; inform public education and advocacy; and strengthen conference workshops and presentations.
Results: Section 1: Background and user-guide with competencies under 5 domains: Basics of PC, Pain and symptom management, Psychosocial and spiritual, Ethical and legal, Communication skills, Teamwork and professionalism. Section 2: practical examples and signposts to useful resources, including strategies to integrate PC into existing courses, how to do a curriculum review in your setting, teaching and learning strategies for PC as well as mentorship and assessment methods. The PC Toolkit and links to helpful resources are available online through 2 free to access sites for global PC (www.cairdeas.org.uk and www.ed.ac.uk/global-health).
Conclusion: PC competencies can be delivered in different ways within health and social care curriculums using these innovative and creative approaches, which recognise existing or hidden competencies as well as the value of developing new materials. PC education should be integrated as a crucial component for transforming practice and health systems strengthening.
Keywords: Curriculum, integration, palliative care, toolkit
PP/11/14: End of Life Care: Perceived Needs of Spouse Caregivers of Persons Living with Motor Neuron DiseaseWarrier GManjushaThomasPriya TreesaANalini1RajaramPrakashiDepartment of Psychiatric Social Work, Bengaluru, Karnataka, IndiaDepartment of Neurology, National Institute of Mental Health and Neuro Sciences, Bengaluru, Karnataka, India E-mail: priyathomasat@gmail.com
Motor Neuron Disease (MND) is a progressive neuromuscular disorder that can have significant and debilitating impact on the affected patient and families. Caregiving of the patients with MND especially during the advanced stages can be quite a difficult task. Few studies have looked into the perceived needs of the spouse caregivers, especially in the socio cultural scenario that is unique to India.
Aim: To understand the perceived needs of spouse caregivers of patients with Motor Neuron Disease (MND) during the advanced stage of illness.
Method: A cross sectional qualitative exploratory study was performed among fifteen spouses of patients diagnosed with MND (Both Males and females) who were receiving treatment from a national tertiary referral centre for Neurological disorders. All the patients were diagnosed as Definite MND according to the El Escorial Criteria. Mean age at onset of illness patients in this group was 51.6. Mean duration of illness at the time of presenting to hospital was 12 months. Functionality of the patient was assessed with Functional Rating Scale Revised: (ALSFRS- R). With the caregiver, interviews were conducted with semi structured interview guide (prompts) to understand their perceived needs at advanced stage of illness.
Results: The preliminary analysis showed that Functionality (ALSFRS) deteriorated at the advanced stages of illness and the caregivers’ perceived needs changed along with the illness progression. Further results and the implications of the study will be presented.
Conclusion: Caregiver of the patient diagnosed with degenerative illnesses in the advanced stage needs to be prepared about the recognition of end of life issues, the tasks that might arise during the advanced stages and a support to handle those issues. Spouse caregivers’ perceived needs during the advanced stage of illness should be addressed. They should have a thorough understanding about what to expect s the condition progresses and should be involved in the advanced care plan. A conceptual framework for intervention with spouse caregivers of patients diagnosed with MND during the advanced stage of illness will be discussed.
Keywords: Caregiver needs, end of life care, motor neurone disease
PP/11/15: Identifying People Who Need Palliative Care Services in the Field Practice Areas of Urban Tamil Nadu: A SurveyESugunaVVinayagamoorthyRMuruganandhamTThirunavukarasuARDongreDepartment of Community Medicine, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India E-mail: drsuguna.e@gmail.com
Background: The Department of Community Medicine at Sri Manakula Vinayagar Medical College and Hospital, Pondicherry has initiated Community Based Palliative Care Program in the four adopted villages under Urban Health Training Center (UHTC), Villupuram. As a part of the program implementation, we felt that it was necessary to identify people in all age groups who need palliative care services.
Methods: A cross-sectional survey was conducted in the four villages under UHTC between January to March 2016. A house to house survey was conducted in the community by a trained team using a structured questionnaire. The respondents were interviewed after obtaining written informed consent. Data were entered and analysed using Epi Info software version 3.5.3. Frequencies and percentages were calculated.
Results: Out of the total population of 22000, we collected details about 6955 individuals by interviewing 1499 respondents. Out of them, 51.8% were male and 48.2% were female. It was assessed that 89.3% of the households were found to be below poverty line. Our survey results showed that 4 individuals (0.06%) were bedridden, 21 (0.3%) were unable to go for work due to chronic incurable illness and 24 (0.3%) were dependent on others for their ADL due to their chronic incurable illness. A total of 24 individuals (0.3%) satisfied atleast one of the three criteria used for assessing the need for home based palliative care services.
Conclusion: Our survey generated data about the number of individuals (24) who need home based palliative care services in the four villages under UHTC, Villupuram. This data will be used for allocation of resources and further to plan the home care visits under community based palliative care program.
Keywords: All age groups, home based palliative care, need, people
PP/11/16: Quality of Death in Advanced Cancer Patients and Bereavement Support to Their Family Members during Home Visits in the Neighborhood of ChennaiTNVijaya1BalakrishnanKalpana2HussainAzhar1VeeraiahSurendren3Department of Pain and Palliative Care, Chennai, Tamil Nadu, IndiaDepartment of Anaesthesia and Pain and Palliative Care, Chennai, Tamil Nadu, IndiaDepartment of Psycho Oncology, Cancer Institute (Wia) Adyar, Chennai, Tamil Nadu, India E-mail: vijayatn@yahoo.com
Background: According to the Economist intelligence unit ranking of quality of death around the world India stands at an abysmal 67 out of 80 countries ranked. This made us think of the type of death and bereavement issues in our home care patients. The present study aims to report on pain management as an indicator of quality of death and the bereavement issues of family members of advanced cancer patients.
Methods: Patients (n = 80) with advanced cancers, irrespective of socio-demographic characteristics, reporting to Pain and Palliative Care Department of Cancer Institute (WIA), Chennai, for symptom management were included in the study. The information was gathered through clinical interviews and case in-take forms, on which the follow-up details were documented. The information was analyzed descriptively.
Results: Of the 80 patients, 62.5% were females with a mean age of 60.49 years. 41% of the patients had painless death and 40% of patients died with mild pain. Only 19% of the patients had a painful death. 60% of the patients were from lower socioeconomic status and they were found to have more bereavement issues as compared to the patients belonging to the higher socioeconomic status. Majority of the patients expired at home (96.3%). Nearly 65% of the caregivers were children, majority of whom did not face any bereavement issues. 61.3% of the patients had accepted their death. It was found that nearly one-third of the patients had no social and financial support.
Conclusion: Most of the patients expired at home as per their wish. Pain was well managed through morphine, other analgesics and psychological support at their homes. Death as such was less stressful due to various palliative care management factors.
Keywords: Bereavement, cancer death, pain, palliative
PP/11/17: Psychological Aspects in Palliative CareJoseJubin PVolunteer, NSS Unit, GHSS, Thrissur, Kerala, India E-mail: jubinpjose94@gmail.com
Palliative care is the area where progression of a disease is minimizing and relieving undesirable symptoms for as long as possible, rather than attempting to cure the incurable diseases.
The functions of palliative care closely related with the psychological aspects. Methods of psychology like changes or varies the events which are hypothesized to have an effect, keeps other conditions constant, and looks for an effect of the change or variation on the system under observation influences palliative care helps.
Each palliative care worker acts as a psychiatrist as well as psychoanalyst for the betterment of beneficiaries. Psychiatrist often are available for prescribing medical treatment when needed, Psychologists do a large part of the professional work of diagnosis and treatment. Palliative care worker should change their role according to the client's will. The supporter of palliative care should be a good listener, acting as a mediator, facilitator, guide, advocate, expert, therapist, promoter and motivator.
Palliative care takers, we should have to be taken care about the people who are suffering from incurable diseases and afflictions through counselling, social and developmental psychology. The counselling psychologists generally work with people who have milder emotional and personal problems. The primary focus of social psychology is on understanding how individuals are affected by other people. Developmental psychologists try to understand complex behaviors by studying their beginnings and the orderly ways in which they change with time.
Palliative care unit helps the people to gain more happy death than stressful one. It makes possible through the frequent interactions and concerns given to the clients. Nowadays people are wealthy and are ready to spend money for their beloved ones. Here, the problem is that incurable diseased and afflicted people need more care and sense of belongingness. They wish to die while seeing their relatives rather than die in ICUs or CCUs without the presence of their relatives.
Keywords: Counseling, psychologist, volunteer
PP/11/18: An Analysis of Referral Pattern to Palliative Care ClinicTDivya1BalakrishnanKalpana2HussainAzhar1TNVijaya1VeeraiahSurendren3Department of Pain and Palliative Care, Chennai, Tamil Nadu, IndiaDepartment of Anesthesiology and Pain and Palliative Care, Chennai, Tamil Nadu, IndiaDepartment of Psycho Oncology, Cancer Institute (Wia) Adyar, Chennai, Tamil Nadu, India E-mail: divyatdsj@yahoo.co.in
Background: Palliative care is an integral component of cancer care and as such we would expect an early referral to palliative care department in a tertiary cancer Institute. Working in a tertiary referral cancer centre we decided to look at the time gap between admission of patients for cancer treatment and referral to palliative care.
Objectives: To improve the quality of life of patients by way of improving the referral system.
Methods: Data was collected from the hospital registry of the first consultation of advanced cancer patients and the date of referral to palliative care unit over a period of six months retrospectively.
Results: Out of 396 patients analyzed 209 (52.8%) were male and 187 (47.2%) were females. The mean age was 52.94 (SD ± 14.007). Majority (n = 235) of patients fall under late adult category. Most of them were diagnosed with head and neck cancer 102 (25.8%), and reproductive system cancer 88 (22.2%). At follow up 204 (51.5%) were alive and 192 (48.5%) were dead. Among this dead patients, 180 (45.5%) died within 6months from the time of registration at pain and palliative care clinic. Many of the patients (51.5%) were referred to pain and palliative care clinic below one year from the time of their registration at hospital.
Conclusion: Proper early reference to the palliative clinic will reduce the disease burden of the patients and their families. We should change the thinking process of medical professionals including oncologists who think palliative care is for pain management and end of life support.
Keywords: Advance cancer, death, palliative care referral
PP/11/19: Identifying Barriers for a Palliative Care Team to Initiate Spiritual ConversationsNaikVinay AThatteNandini NDepartment of Palliative Medicine, Cipla Palliative Care and Training Center, Pune, Maharastra, India E-mail: vinay.naik@ciplacare.com
Background: Patients discuss a myriad of issues with the treating team, including those that may not fall in the medical realm. Medical professionals are comfortable with medical issues since they are within their core competence, but may hesitate to discuss those far out of medicine. This study seeks to examine the barriers that a palliative care team faces in initiating or participating in such discussions.
Method: We conducted this study at a Palliative Centre among the Palliative Care Team involved in core patient care. Participants were selected randomly using a lottery system. Data were collected using semi-structured interviews for eligible participants, after acquiring informed consent. The interviews were digitally recorded and transcribed verbatim post which they were analyzed for themes. This study aimed to identify and highlight barriers perceived by a Palliative Care Team to initiate spiritual conversations with patients.
Results and Conclusion: Incongruity in spiritual belief systems leading to interpersonal dissonance, subjectivity of the experience, and being unenlightened in the spiritual context were some of the reported barriers in this study. These challenges are best addressed with a targeted training approach blended into mainstream programs.
PP/11/20: Review of Community Based Palliative Care Services Initiated at the Urban Field Practice Area of a Medical College in Puducherry from Various Stakeholders’ Perspective - A Qualitative ApproachVVinayagamoorthyESugunaRMurugananthamMRThirunavukarasuDongreAmol RDepartment of Community Medicine, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India E-mail: drvinayagamoorthy@gmail.com
Background: Palliative care is still in its infancy in many places. The last year started community based palliative care services in our urban field practice area at Villupuram, Tamil Nadu following the needs assessment survey.
Objective: To review the home care service, a major component of our community based palliative care, to understand the strengths and challenges from various stakeholders (patients, caregivers, home care professionals) perspective with a view to strengthen and improve the quality of the program.
Method: It is a descriptive qualitative design carried out by the service providers trained in qualitative research methods. In-depth interviews were done among 4 patients, 7 caregivers, 4 social workers, 1 Auxiliary Nurse Midwife, 5 Diploma Nursing Assistant trainees and 12 medical interns for a minimum of 20 minutes. Interviews were audio recorded, transcribed verbatim and content analysis was done manually. Ethical principles were adhered throughout the study.
Results: Descriptive coding of the text information was done, later, similar codes were merged together to form the categories. 4 categories each under strengths and challenges of the home care services emerged out will be discussed in detail. Categories under strengths were physical care, psychological care, social support and teamwork. Categories for felt challenges were interdisciplinary collaboration, volunteer involvement, training enhancement and widening the services.
Conclusion: This review revealed the concerns of various stakeholders. The major part of the service provided deals with psychological care hence training in this regard on communication skill (counselling) is warranted. The other felt concerns like involving community members, availing social security schemes and identifying like minded organisations will be addressed in the program to make the program more acceptable and effective and self-sustainable in future.
Keywords: Community based palliative care, homecare, qualitative review
PP/11/21: Diversion Activity: A Tool to Facilitate Caregiver CopingKhodeVandanaNaikVinay A1Department of Medical Social Work, Pune, Maharashtra, IndiaDepartment of Research and Training, Cipla Palliative Care and Training Centre, Pune, Maharashtra, India E-mail: vinay.naik@ciplacare.com
Background: Diversional activities have different applications including therapeutic ones. As a therapy, it supports, challenges and enhances the psychological, spiritual, social, emotional and physical well being of individuals. This approach can be used to facilitate coping in patients and families facing life limiting conditions. This case series seeks to highlight the impact of Diversional Activities in individuals within a Palliative Care setup.
Method: Experiences of spouses of three patients as observed by the Social Worker were documented. The patients along with their respective spouse attended Musical programs during their stay at the Centre which was an average 50 days. The couples were from different socioeconomic backgrounds. The caregivers had their own set of challenges that compounded caring for the patient.
Results and Conclusion: Attending musical program, helped resolve interpersonal conflicts between the couples by helping refocus on the positive aspects of their relationship. It helped improve caregiving, dealing with anticipated loss and instilling a sense of purpose in the spouse. Incorporating diversion activities as therapeutic interventions in mainstream Palliative Care could potentially add a new dimension to holistic patient care.
PP/11/22: Trans Mucosal Ketamine for the Relief of Cancer Wound Dressing Pain in Patients with Oral CancerPageNivedita DNirabhawaneVivek SGhooiRavindra BDepartment of Palliative Medicine, Cipla Palliative Care and Training Centre, Pune, Maharashtra, India E-mail: ravindra.ghooi@gmail.com
Background: Cancer pain is by itself a challenging entity to manage, as it is multidimensional. Pain during cancer wound dressing is even more distressing. This incidental pain involves inflammatory pain due to mechanical stimulation of raw areas, neuropathic pain due to exposed free nerve endings and nociceptive pain due to tissue manipulation. Patients with oral cancer need to undergo this ordeal once or twice a day, which greatly reduces their quality of life. Lack of patient co-operation due to agony caused during dressing often leads to inadequate cleaning, development of infection, foul smelling discharge, maggots etc.
Material and Methods: 20 oral cancer patients with wounds requiring dressing were included in the study. Average pain score of greater than 4/10 over the last 4 dressings and a baseline score of less than 4/10 was the major inclusion criteria. Patients with distant metastases, major comorbidity, life expectancy less than 1 month, uncontrolled pain and not consenting to the study were excluded. After explaining the procedure and obtaining a written informed consent, patients received transmucosal ketamine 1 mg/kg, 10 minutes prior to dressing. Pain score and vitals were monitored during dressing and after.
Results: Transmucosal ketamine causes a significant reduction in the mean pain score during dressing without causing any adverse drug reactions. The quality of dressing and cleaning of wounds was rated to be qualitatively superior than that done without ketamine. No adverse events were noted during the use of ketamine.
Discussion: There is a need for an analgesic that can manage multifactorial pain during cancer wound dressings. Results suggest that transmucosal ketamine could become the mainstay of incidental pain management.
Keywords: Cancer wound dressing, incidental pain, ketamine, pain management, palliative care
PP/11/23: Dietary Support towards End of LifeBoroseGeetanjaliDietician, Cipla Palliative Care and Training Centre, Pune, Maharashtra, India E-mail: ravindra.ghooi@gmail.com
Background and Purpose: Diet is an important determinant in both health and disease, it has even greater importance, in cancer where cachexia needs to be prevented and treated. Balanced nutrition can make the world of difference for such patients, but may not be available to patients treated at home.
Description of Research Method: The diet of in-patients at Cipla Palliative Care Centre is guided by a dietician, while that of those under home care is not. The food intake of patients admitted to the centre and those receiving care at home was compared. Using a food frequency questionnaire and three day diet recall, the diets were analysed for calorific and nutrient content.
Results of Research: The diet of home care patients is driven mainly by patient related factors such as anorexia, nausea and dysphagia. The diet of those at the centre is modified to take care of these factors, and hence superior in terms of calorie and nutrient content than that of those at home.
Discussion: There is need for dietary management of home care patients, in order to bring them at par with in patients at the centre. The results of this preliminary study suggest the need for a larger study to examine the impact of diet on patients at end of life.
Keywords: Cachexia, calorie intake, end of life, nutrition
PP/11/24: Family Training: Training for Empowerment of Family Members and CaregiversPPSunithaCommunity Resource Center in Palliative Care, Malappuram, Kerala, India E-mail: sunithapallikkara@yahoo.in
Background: The Palliative Care services in Kerala have identified that quality of patient care can be improved only by empowering the family members and the community in patient care. This programme was conducted by the community based Palliative Care organisations in Malappuram District of Kerala under the auspices of Community Resource center in Palliative Care (CRPC), the training and research arm of Malappuram Initiative in Palliative Care, to empower the family members and community in patient care.
Objectives: (1) To improve the quality of care of the patient through family empowerment. (2) To make the family members evolve as the systematically trained caregivers. (3) To make the caregivers aware that the care of the patient is the collective responsibility of the family.
Methodology: The family training is conducted at four levels: (1) Home based training for all family members of a patient about basic care within one month of registration in the respective palliative care clinic. (2) Regular home visits to train the family members who are the primary caregivers and assess the outcome of training on specific issues (e.g. wound care) using the evaluation format. (3) Community level training for the family members of the patients in a palliative care unit having similar issues (e.g. indwelling urinary catheter). (4) Training for patients and caregivers for issues needing inpatient admission, in the inpatient unit for ten days.
Outcome: In 2016, we had 75 trained family members through Ist level programme, 25 trained caregivers from IInd level programme, 50 caregivers through IIIrd level programme and 15 caregivers through IVth level programme.
Keywords: Community, family, training
PP/11/25: Treatment Satisfaction in Cancer Pain Patients in a Tertiary Care Hospital in IndiaSinghSuraj PalSatijaAanchalMishraSeemaBhatnagarSushmaDepartment of Onco-anesthesia and Palliative Medicine, Dr. B.R.A. IRCH, AIIMS, New Delhi, India E-mail: surajpal26@gmail.com
Introduction: Cancer pain management is a dynamic process. Pain assessment, management, and pain related outcomes are closely interrelated. Several studies have examined pain management outcomes such as pain relief, pain satisfaction and quality of life after adequate pain management. In general most studies have demonstrated that the majority of patients could achieve reasonable pain relief within 15 days.
Objective: To examine treatment satisfaction in cancer pain management in Indian set-up.
Methods: A prospective study was conducted at pain and palliative care clinic in Dr. BRA, Institute rotary cancer hospital, All India Institute of Medical Science New Delhi, India. Validated tool to assess pain intensity with a numerical 0-10 scale, where 0 means “no pain at all” and 10 means “the worst possible pain patients can imagine” was used. Total 200 patients with cancer-related pain (Pain - VAS >4/10) were recruited and followed-up for 3 months at regular intervals. Pain was treated according to the WHO cancer pain management guideline.
Results: After week 1, pain relief was 64% and global satisfaction was 68% of patients after 3 months pain relief was 76% and global satisfaction was 90% of patients. The majority of patients achieved adequate pain relief, with decreasing pain severity and pain interference by week 1, with continued improvement afterwards.
Conclusion: The results indicate that as pain relief is achieved, the global satisfaction of the patients also increase in proportion to the reduction in pain severity.
Keywords: Cancer pain, pain relief, satisfaction
PP/11/27: Ensuring Availability of Opioid Medicines while Minimizing Misuse: A Process Report from MNJIO and RCCKAnjaneyulu1PalatGayatri1RVineela1JacobJean2TMaanasa3Department of Pain and Palliative Care, Mnjio and Rcc, Hyderabd, Telangana, IndiaPediatric Palliative Care, Department of Pain and Palliative Care, Mnjio and Rcc, Hyderabd, Telangana, IndiaPalliative Care Unit, Kumudini Devi Hospice, Hyderabd, Telangana, India E-mail: anjank3@gmail.com
Background: The cultivation, production, manufacture and use of opioids is tightly regulated by the Government of India. There are many complex issues in the procurement of opioids, such as getting a “possession license” and “quota” for a stated time period, an “import license” to allow import into the territory of a state, an “export license” to allow a state to supply the medicine to other states and a “transport license” to allow transport from one state to another. Additional challenges include non-uniformity of rules between different states, involvement of multiple agencies in providing required permission, bureaucratic hierarchy within government departments, and the excessive penalties levied for violations. These challenges coupled with the fear of misuse dissuade many hospitals and practitioners from prescribing opioids to patients who require these medicines for adequate pain relief. This paper describes a process that has helped MNJIO & RCC avoid opioid misuse and diversion.
MNJ Institute of Oncology & Regional Cancer Centre is a Centre of Excellence in the state of Telangana. MNJIO has also been given the status of “Recognized Medical Institution” and has been procuring an annual quota of morphine from 2011 to the present. The Department of Palliative Care sees around 3000 new referrals and approximately 8000 review patients every year. Many of these patients require opioids like morphine and fentanyl for cancer related pain. The department has a system of “triple entry” and “double locking” to ensure that opioid prescriptions are correctly dispensed. Previous prescriptions cannot be used to obtain a refill of medications. The quantity of drug dispensed is strictly restricted and the period to follow up fixed at 15 – 30 days. Furthermore patients are required to return any unused opioid medication at each follow up visit. There is one doctor responsible for overseeing prescribing processes and one designated pharmacy.
Methods: Staff noted the quantity of morphine received in each stock, recorded morphine dispensing in stock register and reconciled daily the return of left-over medication.
Results: No instances of abuse or diversion have been identified till date.
Conclusion: The system followed at MNJIO & RCC has allowed the institution to renew its status annually and obtain permission for the annual quota. While ensuring the availability of narcotics for medical and scientific purposes it is important to prevent their diversion and illicit trafficking. MNJIO & RCC is one example of how this can be achieved.
PP/11/28: Care at the End of Life: A Review of Deaths in HospitalASiewSCMacadenSBoscoABThomasVSSamuelDepartment of Palliative Care, Bangalore Baptist Hospital, Bengaluru, Karnataka, India E-mail: amy_raichur@hotmail.com
Background: Care at the end of life has been a neglected area of care in hospitals. Possible reasons for this include not recognizing dying, the hesitance of medical professionals in withdrawing futile measures, their perceived lack of acceptance and sense of failure; and lack of training in effective end-of-life care. As part of the International Collaborative for Best Care for the Dying Person to improve end-of-life care, a retrospective patient chart review of deaths occurring in the hospital was done to understand the current situation.
Method: Deaths occurring in August 2016 were identified from the hospital's mortality register and charts were reviewed for 15 criteria, based on the Collaborative, including recognition of dying by attending doctor, communication to family, review of medications, prescription of anticipatory medications, continuation of inappropriate treatment and provision of psychological and spiritual support. The results were tabulated and analyzed in Microsoft Excel.
Results: Out of 66, 34 charts were reviewed. Charts excluded were of patients who either were “brought dead” (24) or “died in the emergency room” (4) and 4 charts could not be retrieved. Most deaths occurred in the intensive care unit - 29 (85%) with an average stay of 4 days (range: 6 hours to 20 days). The other 5 (15%) died under the care of the palliative care department in the wards of their choice. It was found that while most patients were recognized as dying by the treating doctor - 25 (74%), many patients were still being aggressively treated including ventilator support - 26 (77%). Most families (77%) were communicated regarding the diagnosis and prognosis but fewer (44%) were informed that the patient was dying.
Conclusion: Early referral to the palliative care team could facilitate good end of life care for dying patients through shared decision-making, good communication, symptom management, and good documentation.
Keywords: End of life care, hospital deaths, palliative care referral
PP/11/30: Participatory Approach to Developing Tools to Assess Patient Experience of Care and Its Impact on Quality of CareSarmaDivyaResearch and Document Associate, Samraksha, Bengaluru, Karnataka, India E-mail: divya.samraksha@gmail.com
Background: Palliative care in the context of HIV involves multiple dimensions. It is important to understand patient's experiences of these multiple dimensions, in order to improve the quality of care.
Methods: Asha Jyoti, a HIV palliative care center in Karnataka developed a tool for seeking feedback from patients on their experiences of care. This tool was developed through a participatory consultation with the care centre staff where they identified different dimensions of care which was critical to their work. Following this, lists of 10 critical dimensions were made. A tool was constructed using these 10 dimensions, and exit interviews were held with all patients at the time of discharge. Suggestions for improvement were also sought. Over a period of 18 months, the tool was administered to more than 600 patients.
Results: The results from these interviews were collated, shared and discussed with the team on a quarterly basis. Elements which contributed to high scores on certain domains were discussed. The team discussed possible reasons for low scores on certain domains and came up with concrete steps to improve patient experiences. Some of the points emerging from the qualitative feedback were also considered for improvement. These processes led to certain improvements in the centre – changing the times when the doctor is available for patients, changes in the food provided at the centre to keep it in line with local food habits, on a quarterly basis and helped in improvement of critical aspects of care.
Conclusion: A participatory approach assessing quality of care, where the care team is involved in developing and administering tools for assessment of quality and in using the data from the assessment can lead to improvements in the quality of care.
Keywords: Exit interviews, feedback, HIV, palliative care, quality of care
PP/11/31: Understanding Demographic Distribution Pattern in Advanced Cancer Patients at Jiv Daya Foundation Supported Centers in IndiaPatelAmitkumar1SaneSarika2RautSonal3Dallas Based Grant Manager, Dallas, Texas, USAMumbai Based Project Manager, Dallas, Texas, USADallas Based Medical Grant Coordinator, Jiv Daya Foundation, Dallas, Texas, USA E-mail: ssane@jivdayafound.org
Background: Since 2010 Jiv Daya Foundation - US based Non-Profit Organization has been helping in capacity building by supporting salary of physicians, nurses, social workers, counselors and data managers to implement and improve palliative care services in more than 20 Regional Cancer Centers and Trust Hospitals.
Methods: Data were collected in IcanR database for patients registered for palliative care services at each hospital where staff was supported by JDF. Data was analyzed for demographic factors using IcanR database and excel sheet.
Results: A total 16330 patient's data were collected from the 20 centers between January 2015 and November 2016. East - 3877 (23.7%), North - 5788 (35.4%), South - 4071 (24.9%), West - 1611 (9.8%). With a overall Male to female ratio of 1.37:1. Gender ratio was found to be similar across all four regions (East- 1.4: 1, West- 1.5:1, South- 1.5:1, North- 1.3:1). The most common cancer among women were breast (20.81%), head & neck (13.30%) and cervical cancer (11.03%); whereas head & neck (30.85%), lung (18.16%) cancers among male. Gallbladder cancer incidence was higher in females (10.2%) when compared to male (4%).
More than half (N = 10,443, 59.92%) patients had a cancer between the age of 19 and 60. Overall 545 (3.13%) patients were pediatric (age below 18) and geriatric (above 60) patients comprised of more than one third (N = 6440, 36.95%) of total patient.
Conclusions: The distribution of cancer cases vary across gender. Overall cancer burden in female population is different than the male counterpart. Palliative care should be more specialized at the centers were number of pediatric and geriatric patients are high.
Keywords: IcanR, Jiv Daya Foundation, palliative care
PP/11/32: Professional Oral Care Services in a Specialist Palliative Care Setting in a Hospice in South IndiaWarrierSreedeviMedical Officer, Department of Pain and Palliative Medicine, Pallium India, Thiruvananthapuram, Kerala, India E-mail: drsreedevi@palliumindia.org
Background: Magnitude of oral problems in Palliative care is significantly high. They appear mostly in the form of oral pain, dry mouth, candidiasis, mucositis etc. with pc extending beyond term cancer care emphasis on the importance of oral care in Palliative care patients as it has a great impact in improving quality of life of patients.
Method: Pallium India has started a professional oral care service provision. The service was offered to all the patients registered under our care. Patients are referred by any member in patient care team. The. Study design was case series and descriptive statistics are presented.
Results: Twenty (12 male) patients accessed the oral care services. Both cancer and non-cancer patients accessed the service and the age ranged from24-75 years. Pain was the most common symptom for seeking oral care. 80% (16) of them had pain relief; 10% (2) of patients reported that they could start chemotherapy without any delay; 5% (1) reported prevention of trauma to tongue and interestingly improved chewing and improved self- confidence were also reported. Although we could identify oral needs among children with cancer through a routine oral check -up, we could not provide any treatment due to lack of referral and protocols. Procedure for one child with Downs Syndrome is awaiting anaesthetic work up for treatment.
Conclusion: Organizations with specialist palliative care services should consider offering professional oral care services due to the need and potential improvement in symptoms. Developing protocols for oral care in palliative care patients including those with relative contraindications, thereby improving referrals will be the way forward for scaling of services.
Keywords: Oral care, specialist palliative care, symptom management
PP/11/33: Gender-wise Association of Daily Opioid Doses in Cancer Pain PatientsShekharVarunBhatnagarSushmaGuptaRitu1SatijaAanchalDepartment of Onco-anesthesia and Palliative Medicine, AIIMS, New Delhi, IndiaDepartment of Laboratory Oncology, Dr. B.R.A. IRCH, AIIMS, New Delhi, India E-mail: varunshekhar18@gmail.com
Introduction: Pain is common and often most dreading symptom that limits quality of life of patients with cancer. According to World Health Organisation (WHO), about 60-90% of patients with advanced cancer suffer from pain. For cancer pain management, WHO pain relief guide is conventionally followed which indicates opioids use for managing moderate to severe pain.
Objective: To examine the association of 24-hour morphine doses with age, gender and cancer diagnostic category.
Methods: A cross sectional study was carried out at pain and palliative care clinic in Dr. BRA, Institute Rotary Cancer Hospital, All India Institute of Medical Science New Delhi, India. Total 250 patients who were taking morphine since at least one month were enrolled in this study and were divided into two group-responder and non-responder to morphine based on the pain relief with morphine. The 24-hour doses and clinical data of patients were recorded. The association between age, sex and cancer diagnostic categories and 24-hour morphine doses; and association between age, sex and cancer diagnostic categories and responder non-responder group were statistically analysed using Wilcoxon rank-sum (Mann-Whitney) test (STATA 11 software).
Results: Significant higher 24h-morphine doses were observed in non-responder group and male (P = 0.0012 and P = 0.0392 respectively). Significant association of 24-hour morphine doses was found for sex and non-responder groups.
Conclusion: The present study highlights the association of gender with the total opioid doses in cancer pain patients in Indian scenario.
Keywords: Cancer pain, gender, opioid dose
PP/11/34: Establishing a Palliative Care - Link Nurse Program – Process and OutcomeManuelAthul JosephDanielSunithaVenkateswaranChitraSinghCharuDepartment of Palliative Medicine, Amrita Institute of Medical Sciences, Kochi, Kerala, India E-mail: athulmanuel@gmail.com
Background: Understanding and acceptance of palliative care is still limited. In an acute tertiary care hospital, palliative care becomes low priority for doctors and nurses when they are focussed on curative treatment. There is evidence (Rogers et al, 2000) that identifies deficiencies in the basic nursing care of dying hospital-based patients as well as problems relating to communication with patients and their relatives. It is imperative that the majority of nurses receive some education in palliative care, particularly as health-care systems become more accountable and transparent. The intent of the program was integration of palliative care into mainstream medical practice by training nurses to be resource persons within nursing teams in different wards. The expectation was also for postgraduates to be guided for initiating palliative care referrals.
Methodology: Nurses with an interest in palliative care and intention to be trainers were criteria for selection. The program was run in association with the In-house training program for nurses. Steps were taken through the Nursing and Medical administration to empower nurses to initiate a referral to palliative care on identification of trigger symptoms.
Training was conducted for: (1) Palliative care principles. (2) Use of opioids and other medication. (3) Principles of symptom management. (4) Palliative care nursing. (5) End of life care. (6) Ethical principles underlying palliative care. Evaluation of nurses was done through a pre and post training questionnaires and repeat evaluation after 6 months.
Outcome: To provide a formal mechanism for the delivery of Link Nurse education, training and support that will promote best practice palliative care and cross organisational communication and relationship building.
Results: The pre and post course evaluation showed a significant improvement in the level of knowledge and confidence in all the topics covered.
Keywords: Education, nurse role, palliative care
PP/11/35: The Need for Regular Pain Assessment and Monitoring as Part of Comprehensive HIV CareYecharappaSharadaBillalliShafiulla HSarmaDivyaMullaSaffiullaAnehosurAnnaraoKSulekhaPalliative Care Center, Samraksha, Koppal, Karnataka, India E-mail: sulekha@samraksha.org
Background: With the emphasis on anti-retroviral treatment, pain control and management is frequently not acknowledged as an issue in HIV care. However, people with HIV suffer different kinds of pain both as a result of their illness and the medication.
Methods: Asha Jyoti in a HIV palliative care centre, operated by Samraksha in Karnataka. Here regular pain assessment is done for all patients at specific intervals, and even after discharge, there telephonic follow up is done, if patients report some lingering pain at the time of discharge.
A review of all patient files over the last 18 months was done to assess levels of pain at the time of admission and discharge.
Results: Over 68% of the patients reported pain levels between 8 to 10 at the time of admission. The nature of pain was different – pricking, numbness, tingling, burning, colicky. Location of pain was also varied – abdomen, limbs, feet, joint, chest and headache.
At the centre, pain assessment was done twice a day in the initial phase. After three days, if the pain was decreasing, the assessment was done once a day. Dosages were modified based on the assessment.
The regular assessment and modification of medication and dosages helped in relieving pain for most patients. Around 58% reported no pain at the time of discharge. 26% reported pain levels of 1 to 2, 5% of 3-4. 9% had pain levels of over 5 at the time of discharge. Pain assessment continued over phone for these people, and this was done twice a week.
Conclusion: Pain remains a major issue for people living with HIV. Frequent pain assessment is critical for treating this pain. The services need to be able to make these assessments frequently and change the interventions accordingly.
Keywords: HIV, pain assessment, pain management
PP/11/36: Palliative (Pain) Management in Cancer Patients by Nonconventional and Noninvasive MethodsDesaiMadhav GShahHiralMathewKandathilPoteAnilPoteTruptiWalwaikarPradeepNavjeevan Global Health Center, Mumbai, Maharashtra, India E-mail: hiralshah13@icloud.com
Summary Background: Fastest Pain management in Cancer patients (of any stage with or without metastasis, treated by conventional methods or untreated) is the objective of this research. Non conventional, non invasive, minimum chemical and natural methods are selected along with specific diet and specialized exercises. They are found compatible with conventional medicines and do not interfere with ongoing chemo, radiation etc. This study assessed fast improvement in pain within few hours to few days.
Old Indian Science is the basis of this study, of herbs, molecules, ions, their effects on body as a whole and in turn the disease conditions in general and in specific. The study also includes the combination of commonly used herbs in Ayurveda and Homeopathy combined with allopathic forms of vitamins and minerals. Considering in mind the low immune systems, poor digestion, surgeries, heavy chemical medicines already been taken during cancer treatment, special consideration was given in selection of natural ingredients, food and food extracts and minimum chemical based ingredients.
Pain: Pain is studied from many angles. An extensive and deep study is carried out for last 20 years, studying minor stomach ache due to gas to metastatic stage pain of scale 10 was the span of pain cases undertaken. The study showed many interesting outcomes. Medical Observations and continuous patients feedback played a key role in filtering specific pain causing and pain relieving food, food ingredients, herbs, minerals. Vitamins which are selected for the study. The study observations shows that body reacts very fast with pain causing agents, may it be food or herb or chemicals. Many a times there are instant increase in the pain scores. In few minutes to 48 hr span the pain scores can rise by double due to specific pain causing agents. The study also showed that supplementing essential vitamins and minerals can bring down the pain scores considerably. Clinical study of supplementing, sodium, calcium, zinc along with Vitamins A, E, D in different dilution in combination with specific selected foods and herbs.
Following herb tincture, herbs and ingredients are selected from homeopathy and Ayurveda due to their established usage as soothing and pain relieving effects, after filtering from a bunch of herbs and other natural ingredients.
The active ingredients of our medicines are (1) Arnica Montana. (2) Extracts of wild oats. (3) Praval Bhasma from Ayurveda. (4) Curcumin. (5) Vitamin D3, Vitamin C, Vitamin E. (6) Calcium compounds, (Succenate, Gluconate, Carbonet). (7) Sodium compounds, Zinc compounds, Magnesium Compounds (Carbonate, Cloride). (8) Diluent used is Fennel seed powder extract, The combinations and grammage differ with the different patients, complaint wise and different body presentation and sign symptoms (SS) wise.
Findings: Between May 2011 to October 2016 about 160 Cancer patients were under Navjeevan Palliative (Pain) Care. The findings showed varied results with about 80% of patients getting remarkable effect on pain within few hours to 1 week interval. Pain of Scale 10, 9, 8, 7 came down to below 3. About 10% of patients took more than two weeks time for effective pain relief. About 5 to 7% of patients took more than 3 weeks. About 3 to 5% of patients did not report back ? Results are not known.
Interpretation: Fastest, (many a times instant) relief in pain in Cancer patients.
Keywords: Alternative medicine, herbal medications, symptom management
PP/11/37: An Experience of Initiating Palliative Care Unit at Aarupadai Veedu Medical College and Hospital, PuducherrySKirubakaranDArunachalamPalliative Care Unit, Aarupadai Veedu Medical College and Hospital, Puducherry, India E-mail: kirubasam01@gmail.com
Objectives: (1) To find out the type of cancer patients attended our Palliative Care Unit. (2) To assess the Malignant pain intensity and the length of hospital stay of the Cancer patients those who admitted in AVMCH for Palliative Care.
Materials and Methods: The Palliative Care Unit was initiated in AVMCH on June 1st 2016. A Palliative Care team comprising of IAPC trained Palliative Physician and Nurses take cares the OPD and admit the patients in the respective ward based on the diagnosis. The cancer patients for Chemotherapy and Radiotherapy apart from Palliative Care are referred to Regional Cancer Centre. The Numeric Rating Scale (NRS) was used as the fifth vital sign to assess the pain intensity. The statistical analysis was done using the percentages for type of cancer and Median for the length of hospital stay.
Results: Total 75 patients attended Palliative care unit in last 6 months. Out of which 23 (30.7%) were Cancer patients. Among them 5 (21.7%) were cervical cancer patients and 4 (17.3%) were Carcinoma Prostate, Carcinoma Buccal Mucosa and Carcinoma stomach respectively.
Based on the pain intensity of the cancer patient, length of hospital stay in days were analyzed the Median of 2 days were the hospital stay for the patients with 0-3 pain intensity, Median of 4 days were the hospital stay for the patients with 4-7 pain intensity and the Median of 6.5 days were the hospital stay for the patients with 8-10 pain intensity.
Conclusion: It was found that patients with severe pain intensity tend to stay longer in hospital. Hence the capacity building among the multidisciplinary doctors and community motivation will add more capitalization of the palliative care unit initiation at institutional level.
PP/11/38: The Utility of Silver in Palliative CareSVatsalaSeshacharPrabhaAnandJulietDepartment of Palliative Medicine, Kidwai Memorial Institute of Oncology, Bengaluru, Karnataka, India E-mail: svatsala2009@gmail.com
Silver is a nontoxic, healing metal having antimicrobial activity. It is a natural antibiotic, to which microbes do not become resistant in course of time, unlike chemical antibiotics. To exert the antimicrobial activity, a small quantity in ppm level is enough. Carl Nageli a Swiss botanist worked on this aspect of silver in 1893. He called this effect as oligo-dynamic effect. (oligo-few, dynamos-power).
The use of silver and its compounds in medicine is not unknown. Sticks of silver nitrate with potassium nitrate are used for cauterisation to stop bleeding and also to remove unwanted growths like warts. It is used in amputational cauterisation. Dentists use silver amalgam to fill dental cavities. Very dilute solution of silver nitrate is used in the eyes of infants to prevent infection. Silver sulphadiazine is used for burns.
Colloidal silver solution (CSS) can be prepared by electrolysis which is a cost effective, sure healing agent. However available commercial samples in UK and USA are prohibitively expensive. Patients undergoing chemo/radiation therapy suffer from oral mucositis, a debilitating complication of the treatment. When CSS is kept in the mouth for 15-20 minutes without swallowing appreciable relief happens and they are able to eat even spicy food happily, soon after. In patients suffering from burning sensation, itching, discharge, malodour from vagina, homemade tampons soaked in CSS and inserted brings tremendous relief in 15-20 minutes. Fine silver and charcoal powders mixed with isabgol, is found to be very effective in controlling the malodour of the cancerous wounds and also helps in relieving the pain.
PP/11/40: Role of Emergency Home Care Service in Palliative Care – Alpha Palliative Care ExperienceTJJose BabuMMSunilkumarDepartment of Pain and Palliative Care, Alpha Palliative Care, Edamuttam, Thrissur, Kerala, India E-mail: drsunilkumarmm@rediffmail.com
Background: In Kerala, most of the Palliative Care services are designed to provide care at home or in a hospital/hospice. Mostly the homecare services are provided during daytime from 9am to 3.30PM. Alpha Palliative Care works as Hospices and Link Centers. Alpha Palliative Care Link Centers work in an area of Block Panchayath working from 9am to 5pm. We have such 10 centers in Thrissur District. When a patient has a problem, the caregivers usually wait till evening hoping that it will be resolved. As evening approaches, they panic and start calling to get services by evening. In order to care for these patients, Alpha Palliative Care has implemented an emergency home care services from 3 PM to 8 PM.
Method: This will be a survey of the emergency homecare service. All the emergency home care case sheets between 7th November 2016 to 31st January 2017 will be reviewed and the reason for emergency home care will be tabulated.
Results: Shall be published during conference
Keywords: Emergency care, link centers, out of hour service
PP/11/41: Does Seeing Death Everyday Reduce Death Anxiety in Nurses?Prabha SLakshmiCJothimaniBalasubramaniLathaNarayanAnandValavadi Naryanaswamy Cancer Centre, GKNM Hospital, Coimbatore, Tamil Nadu, India E-mail: prabhasujith@yahoo.com
Introduction: Death anxiety is the morbid, abnormal, or persistent fear of one's own death. Nurses often exposed to death during their work may also have death anxiety. This may affect both their professional and personal life.
Aim: To compare the level of death anxiety among nurses caring for patients in oncology & critical care with general wards in our hospital.
Materials and Methods: The Tembler's Death Anxiety Questionnaire was administered to 75 nurses working in the oncology & critical care and general wards in our hospital.[1] This is a 15 point questionnaire with scores of 0, 1, 2 in 4 different aspects death anxiety. Fear of the unknown; fear of suffering; fear of loneliness; fear of personal extinction are assessed.
Results and Discussion: Demographic data showed that there was no difference between the two groups, except for work experience. Nurses working in oncology & critical care (Group A) had more years of work experience compared to nurses working in general wards (Group B). The death anxiety score ranged from 14.1 to 14.9 amongst the two groups and the mean was 14.4. There was no significant difference in death anxiety among the two groups. Our study also showed that irrespective of their work area, all nurses had a death anxiety score significantly higher than the population mean (p < 0.001). The most significant variables were fear of personal extinction (p < 0.006), fear of loneliness (p < 0.026) which were statistically significant in the two groups.
Conclusion: Our study revealed that the anxiety regarding death was high amongst nurses working in our hospital irrespective of their department. This may well be an unmet need which may need to be addressed.
Keywords: Anxiety, death, nurses
R<sc>eference</sc>ConteHRWeinerMBPlutchikRMeasuring death anxiety: conceptual, psychometric, and factor-analytic aspectsJ Pers Soc Psychol19824377585PP/11/42: Quality of Life Assessment in Breast Cancer SurvivorsChinnasamySwarnalakshmiNVijilakshmiArumughamRajkumarPArulrajMurugaiyanNagarajanNarayanAnandValavadi Naryanaswamy Cancer Centre, GKNM Hospital, Coimbatore, Tamil Nadu, India E-mail: drrajkumar@gknmh.org
Aim: To assess the quality of life in breast cancer survivors treated at a single Institution.
Background: Breast cancer is the most common cancer among women in the western world and in India as well. Advancements in treatment have led to more number of patients being cured of the disease. Despite being cured of the disease they continue to suffer from the long term consequences of both the disease as well as the treatment. Quality of life (QOL) continues to be an area of concern in such survivors. In India, the number of studies that assess QOL is far and few. Hence, this study was done to assess the QOL in breast cancer survivors who were treated at our centre.
Materials and Methods: The study population included breast cancer survivors who were free of disease and with a minimum follow-up of 1 year. Patients treated at other centers but on follow-up at our centre were excluded. A self administered questionnaire –EORTC FACT-B was administered. It consisted of 40 questions pertaining to 5 categories of QOL-physical, social, emotional, functional and additional concerns. Scoring was done on a 5 point scale with a higher score indicating better QOL. Reverse coded items were re-coded.
Results: A total number of 111 survivors were included in the study. The average age was 52 years and median follow-up duration was 34.5 months. The average score of each of the 5 categories was 3. Among questions related to social well-being, the least score of 2 was for sexual life while family support in terms of emotional support and acceptance had a high score. In the emotional QOL category, most of the survivors seemed to have come to terms with their disease as shown by a high score of 4 for this factor. A low score of 2 when it came to attractiveness and consciousness about their dress implicated this to be an area of concern for the survivors.
An analysis of the possible predictors of QOL like age, stage of disease and adjuvant treatment given had no influence on any of the categories of QOL. Older women had lower scores in the categories of functional and emotional well being. Time since diagnosis had an impact on functional well being, with longer the follow-up better the QOL in this aspect.
Discussion: This study shows that a majority of the patients seemed to have a reasonable QOL of life as a whole in all the 5 categories. The areas of concern were elderly women who had lesser QOL scores for functional and emotional well being. Similarly, sexual well being was low among the survivors probably related to the fact that a diagnosis of cancer is still taboo in the Indian society. Special attention to provide emotional support to the elderly survivors by regular counselling and rehabilitative measures to improve their functional well being should be the focus of care.
Keywords: Breast cancer, counseling, quality of life
PP/11/45: Effect of Physiotherapy on Quality of Life in Pediatric Palliative CareTripathiHimadriMacGamwellHanifeTchukiTenzingKumarAbhishekDinandVeroniqueCanKids Pediatric Palliative Care Centre, New Delhi, India E-mail: physiotherapist@cankidsindia.org
Background: Pediatric Palliative Care aims at improving the quality of life of children with chronic illnesses and their families. Physiotherapy is an important part of this multidisciplinary approach. Physiotherapy practice in community-based settings, such as hospice and palliative care centres, identifies and maximizes movement potential within the sphere of promotion, potential, treatment and rehabilitation. We conducted a pilot study to assess the effect of a physical exercises programme on the physical and functional performance and quality of life in children with incurable cancer and short life expectancy.
Method: A prospective study was conducted on children admitted in the hospice-based Pediatric Palliative Care Programme of CanKids, Delhi. All children suffered from advanced, refractory or relapsed cancer and received holistic palliative care, besides cancer-directed therapy for some. The course of physiotherapy treatment, provided 4-5 days a week, was assessed prospectively over a period of 180 days. Medical condition was recorded, including respiratory status, fatigue, pain, constipation, muscle atrophy, limb amputation. Physiotherapy techniques used in each patient were also recorded. Physical performance was measured by Lansky Play Performance Scale; fatigue by PedsQL Multidimensional Fatigue Scale; and strength by Manual Muscle Testing. Repeated measurements were done, and compared with initial measurements.
Results: 35 children (age 3-21 years) with solid tumors and haematological malignancies were enrolled in the study. 12 of them showed significant improvement with physiotherapy. Therapeutic exercises, thermal modalities, soft tissue manipulation, endurance training, respiratory muscle strengthening exercises, and assistive devices improved physical and functional performance.
Conclusion: Physical exercise is a feasible way to improve well being among children with incurable cancer. Considering the scope of physiotherapy in India and in Palliative Care, professionals in a multidisciplinary palliative care team need to understand its importance and to work towards policy changes to successfully implement physical therapeutic palliative care centres.
Keywords: Functional performance, physiotherapy, pediatric palliative care
Ethics; end of life care legislation; life support limitation; palliative carecaregiver burden; elder abuse; patient autonomy