
Translate this page into:
Mediating Role of Affective Experiences in the Relationship between Perceived Social Support and Life Satisfaction among Breast Cancer Patients
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aim:
The role of social support network in managing psychological symptoms in cancer patients is widely acknowledged. The purpose of this study was to investigate the potential mediating role of Affective experiences in the relationship between perceived social support (PSS) and life satisfaction (LS) among breast cancer patients in India.
Methods:
A total of 100 breast cancer patients from S. S. Hospital, Banaras Hindu University participated in the study. They were tested using the PGI Social Support questionnaire, Satisfaction with Life Scale and Scale of Positive and Negative Experiences.
Results:
Co-relational results indicated that PSS was positively associated with positive affect and LS, while inversely related to negative affect. Affect was also associated with LS. Results showed that the mediation of affective experiences in the relationship between PSS and LS was significant (P <.01 level).
Conclusion:
Both PSS played a big role in LS among breast cancer patients. Besides focusing on improvement of the social support network, the psychologists and counsellors should adopt an integrated approach for evidence-based intervention strategies to enhance their ability to effectively balance their positive and negative emotions to promote LS among cancer patients.
Keywords
Affective experiences
breast cancer
life satisfaction
perceived social support

BACKGROUND
Breast cancer leads to many situations that may threaten the psychosocial integrity including changes in patients' personal paths of life including their daily activities, work, relationships, and family roles, and is associated with a high level of patients' psychological stress. This leads to a lack of social or personal control, progressive physical deterioration and the thoughts of near death.[1] The social behavior of women is also affected, leading to restrictions on their social lives and changes in daily life activities, facts that may contribute to depressive behavior and social isolation. Considerable empirical evidence substantiates the importance of social networks and social support to health and well-being among the elderly. Social support refers to mechanisms through which interpersonal relationships protect people from the detrimental effects of stress. It is a key for any individual's emotional safety. The main sources of social support are the spouse, family, friends, neighbors, and other individuals who inter-relate and provide reciprocal support. Considerable evidence links social support with increased health-promoting behavior[2] such as dietary habits, physical activity, smoking habits, alcohol intake, and adherence to medical regimens.[34]
In recent years, there has been a dramatic increase in the scientific study of well-being and positive aspects of mental health[567] and although theoretical models differ in how they define optimal well-being, they all agree that deep and meaningful close relationships play a vital role in human flourishing. A large body of empirical work shows that people who are more socially integrated and who experience more supportive and rewarding relationships with others have better mental health, higher levels of subjective well-being (SWB) and lower rates of morbidity and mortality.[89] Unfortunately, the mechanisms linking close relationships to health and SWB are not well understood. Most of the empirical work linking relationships to health and well-being conceptualizes social relations in terms of individual's general reports of their marital status, social networks social integration and perceived social support (PSS).[910] As a result, we know little about how relationships promote or hinder well-being.
Subjective well-being (SWB), people's cognitive and affective evaluations of their lives, has been an important research area in positive psychology. It is thought to comprise of a cognitive-judgmental domain reflecting life satisfaction (LS) and an emotional evaluation characterized by positive and negative affect, has been linked to the affective domain of SWB.[11] For example, research has demonstrated that happy individuals tend to have larger social rewards, better work outcomes, greater coping abilities, better immune system, to be more cooperative, pro-social and charitable, having satisfying social support and to live longer than individuals who are not happy.[12]
There is strong evidence for the main effects model of social support indicating that strong relationships promote well-being not just as a resource in times of adversity but also by enabling individuals to fully participate in life's opportunities for growth, development in the absence of adversity and satisfaction with life. Consistent with previous research, we found that the different forms of SWB were differentially related to the facets of social support. Specifically, LS was predicted by enacted and perceived support, positive affect was predicted by family embeddedness and provided support, and negative affect was predicted by perceived support.[13]
Perceived support refers to the expectation that support will be provided rather than referring to specific instances in which one has received support. In general, perceptions of the availability of social support have been linked to better outcomes during times of stress.[14] Women with breast cancer sometimes report a lack of balance is perceived when support requested is not provided or when the support provided was not the support sought. Perception of reduced support may be linked to a certain incompatibility between the patient's real needs and the support provided.[15] High levels of anxiety and distress and low positive emotional experiences tend to reduce as one's perception of social support experienced by women undergoing breast cancer treatment due to psychosocial changes. In some cases, women may even elucidate the reception of support as personal incompetence. Distress and depression accruing from the treatment side effects together with perceived support, may affect the psychosocial adjustment of women with breast cancer. In regards to the cognitive-judgmental component of SWB, Newsom and Schulz[16] found that greater PSS was correlated with higher LS and linked to fewer depressive symptoms in older adults.
Several empirical studies have been carried out, indicating that social support was closely associated with affective experience.[1718] Positive feelings reflect the degree to which an individual feels energetic, enthusiastic, cheerful, active and alive and negative affect is depicted as a condition of discontentment, not being joyful, or subjective distress including such feelings of anger, hate, weariness, shame fear and irritation.[19] Affective (emotional) experience could mediate the impact of social support on LS,[20] which implies that the social network and affective meditation models are interdependent. Yet the specific pathways through which perceived support promote optimal well being is not well understood. In addition, to the best of our knowledge, there have been no studies to investigate the relationships between PSS and LS through mediating factor like positive and negative experiences.
Therefore, the primary purpose of this study was to propose and test a conceptual model that explains the interrelationships among those factors to provide a theoretical foundation for identifying the specific interpersonal processes that underlie the effects of close relationships on LS. The secondary purpose was to examine the mediating role of positive and negative affective (emotional) experiences in the relationship between PSS and LS. Based on the previous literature, a conceptual model was created that explains the interrelationships among PSS LS and affective experiences [Figure 1]. To test the validity of the model, we addressed the six research hypotheses on which it relies:
-
PSS will have positive direct effect on LS among Indian breast cancer patients
-
PSS will enhance positive affect among Indian breast cancer patients
-
PSS will reduce negative affective experiences among Indian breast cancer patients
-
Positive affective experiences will enhance LS among Indian breast cancer patients
-
Negative experiences will reduce LS among Indian breast cancer patients
-
Positive and Negative experiences will serve as a mediator in the relationship between PSS and LS.
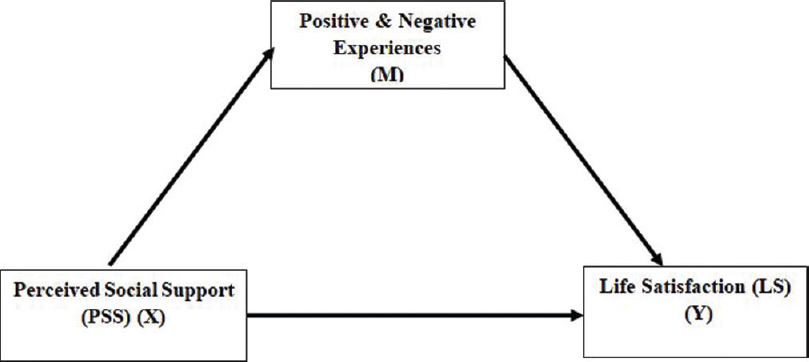
- Illustration of hypothetical model of mediation
The hypothesis model for this study is shown in [Figure 1].
METHODS
Participants
The participants included in this study were 100 women diagnosed with breast cancer and receiving treatment at the Department of Surgical Oncology, Institute of Medical Sciences, SS Hospital, Banaras Hindu University (BHU) Varanasi, India during the period from June 2016 to March 2018 were enrolled in the present study. Patients who were aged below 40 years and above 65 years, or had any comorbidities or psychiatric condition (as indicated by the hospital staff) were excluded. The rationale behind restricting the age range between 40 and 65 years was that patients in this age group having a high incidence of breast cancer in India[21] and usually report similar psychological problems.[22] After obtaining their written informed consent for this study, a set of self-administered questionnaire was distributed to the participants, and the clinical data were collected from their medical records. The protocol of research was in accordance with ethical standards of and was approved by Institution's ethics committee (Reference No.-ECR/Bhu/Inst/UP/2013/Re-registration-2017 dt. 31.01.2017/No. Dean/2017/EC/24.10.2017) the final sample consisted of 100 participants from SS hospital BHU, Varanasi. The average age of the sample was 49.04 years (standard deviation [SD] = 8.30). Forty-seven patients were having up to the primary level of education. More than 50% of the patients were married (n = 89) housewives (n = 73) and belonging to rural areas (n = 61). 68% of the patients were surviving of up to 6 months of illness and most suffering from stage II to stage III of the disease [Table 1].
| Variables | n=100, n (%) |
|---|---|
| Age (years) | |
| 40-50 | 68 (68) |
| 51-60 | 21 (21) |
| 61-65 | 11 (11) |
| Education | |
| 1. Basic reading/writing | 18 (18) |
| 2. Primary-8th class | 47 (47) |
| 3. Metric-Intermediate | 23 (23) |
| 3. Graduate or above | 12 (12) |
| Marriage | |
| 1. Married | 89 (89 |
| 2. Single/widow/divorced | 11 (11 |
| Residence | |
| 1. Rural | 61 (61) |
| 2. Urban | 30 (30) |
| 3. Semi urban | 09 (09) |
| Family income (per month) | |
| 1. Upto 20,000/-INR | 75 (75) |
| 2. >20,000/-INR | 24 (24) |
| Family type | |
| 1. Neuclear | 38 (38) |
| 2. Joint | 62 (62) |
| Employment | |
| 1. Housewife | 73 (73) |
| 2. Self employed | 18 (18) |
| 3. Government/private employee | 9 (9) |
| Duration of illness (months) | |
| 1. Upto 6 | 68 (68) |
| 2. 6-12 | 19 (19) |
| 3. >12 | 13 (13) |
| Stage of disease | |
| 1. Stage 0-I | 46 (46) |
| 2. Stage II-III | 54 (54) |
Tools
Perceived social support
PGI Social Support Questionnaire (PGI SSQ) was administered to assess PSS.[23] Out of the 18 items, 7 are positive worded and 11 are negatively worded. Each item is scored on 5 point scale from “fully” to “not at all” with a high score reflects greater Social support. The Hindi adaptation of PGI SSQ achieves good reliability and validity among Indian Population.[2425262728] The Chronbach alpha found was found 0.67 for the present sample.
Affective experiences
The scale of positive and negative experiences (SPANE) was administered to assess affective experiences.[29] The SPANE is a 12-item questionnaire that includes 6 items to assess positive feelings and 6 items to assess negative feelings. For both the positive and negative items, three of the items are general (e.g. positive, negative) and three per subscale are more specific (e.g. joyful, sad). Overall affect balance score is obtained by subtracting negative feelings scores from positive feelings scores. In this scale, the participants respond to each question using a 5 point Likert scale (from 1 = very rarely or never to 5 = very often or always). The resultant score can vary from-24 (unhappiest possible) to 24 (highest affect balance possible). The Hindi adaptation of SPANE achieved good levels of reliability and validity among the Indian Population.[30] The Chronbach's alpha of SPANE in this study is. 75, which indicates the high reliability of this scale.
Life satisfaction
The satisfaction with life scale (SWLS) was administered to assess life satisfaction. SWLS consists of five statements. Participants will indicate their degree of agreement to these statements using aseven point Likert Scale. The seven-point scale is as follows: 1 = strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = neither agree nor disagree, 5 = slightly agree, 6 = agree, and 7 = strongly agree. The SWLS score is derived by summarizing the rating of each participant for the five statements.[31] The Hindi version of SWLS achieves good validity and reliability.[32] Chronbach's alpha of SWLS in this study is 0.844, which indicates the high reliability of this scale.
Procedure
Participants completed multi-item questionnaires including PGI-SSQ, SPANE, and SWLS. Only those who completed the consent form were allowed to respond to the questionnaires. Participants could answer the questionnaires at their own pace and typically took about 15–20 min to complete all sections. The obtained data were analyzed using descriptive statistics, bivariate correlations and mediation analysis with the help of SPSS version 20. (IBM Corp., Armonk, NY).
RESULTS
Descriptive statistics (mean and SD) was performed to assess the mean of self-reported accounts of PSS, Positive and Negative Experiences and LS. Means, SDs and minimum and maximum scores for each variable are located in Table 2.
| Number | Measures | Mean | SD | Minimum | Maximum | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Positive experiences | 17.96 | 5.72 | 7.00 | 29.00 | 1 | -0.473** | 0.598** | 0.710** |
| 2 | Negative experiences | 15.36 | 5.71 | 6.00 | 28.00 | 1 | -0.420** | -0.426** | |
| 2 | PSS | 54.70 | 9.54 | 37.00 | 83.00 | 1 | 0.448** | ||
| 3 | LS | 17.88 | 7.05 | 5.00 | 33.00 | 1 |
**Correlations significant at 0.01 level (two-tailed). PSS: Perceived social support, LS: Life satisfaction, SD: Standard deviation
Bivariate correlations
Bivariate correlations were analysed to examine existing relationships among study's variables. As expected, PSS was affirmatively related to positive emotional experiences (r = 0.598, P < 0.01) as well as LS (r = 0.448, P < 0.01) while inversely related to negative experiences (r = −0.420, P < 0.01). Consistent with expectations, Positive emotional experiences was highly related to LS (r = 0.710, P < 0.01) while negative emotional experiences were inversely related to LS (r = −0.426, P < 0.01). Overall, all variables were significantly related in the expected direction and to the expected degree. Inter-correlations among study's variables are located in Table 2.
Mediation model
Two mediation models were analyzed in this study, examining the relationship between PSS and dimensions of SWB. The first mediation model examined the indirect effect of positive emotional experiences on the relationship between PSS and LS. While the second mediation model examined the indirect effect of negative emotional experiences on the relationship between PSS and LS. Depictions of all mediation models are included in Figure 2a and b.

- Illustration of mediation between perceived social support and life satisfaction by both (a) Positive affect and (b) Negative affect. Data values are unstandardized regression beta for specific pathways. PSS: Perceived social support, LS: Life satisfaction, PA: Positive affect, NA: Negative affect. *P < 0.05; **P < 0.01
All models were analyzed using Preacher and Hayes'[33] mediation approach. Again Preacher and Hayes'[33] mediation approach is a non-parametric, bootstrapping technique that offers more statistically powerful and accurate results when compared against the traditional approach to mediation modelling. The bootstrapping procedures in SPSS Process macro from the mediation model 4 were used to test the significance of the indirect effects of social support on LS through the mediation of affect balance.[33] Following the recommendations of Shrout and Bolger,[34] we generated 1000 samples from the original dataset (N = 100) via random sampling. If the 95% confidence interval (CI) of the outcome of the mediation effect did not contain zero, then the mediation effect would be significant at the 0.05 level.
In the first model, the unstandardized point estimate of the indirect effect was 0.304, 99% CI = 0.220 to 0.400. The direct effect between PSS and LS became insignificant (t = 0.415; P > 0.05 after accounting for the indirect effect of Positive affective experiences indicating moderate indirect effect. In the second model, the unstandardized point estimate of the indirect effect was 0.089, 99% CI = 0.29–0.18. The direct effect between PSS and LS remained significant (t = 3.41, P < 0.01) even after accounting for the indirect effects of negative emotional experiences, indicating partial mediation.
As shown in Figure 2a, the total effect (β = 0.331, P < 0.01) from PSS to LS was at a significant level (Step 1). Moreover, the direct path from PSS to Positive experiences (β = 0.358, P < 0.01) was significant (Step 2). Meanwhile, the path from the mediator, namely, positive affect (β = 0.847, P < 0.01) to LS was significant (Step 3). However, after inserting mediator in model, the direct path from social support to LS became insignificant (β = 0.027, P > 0.01) (Step 4). Moreover, the mediating variable (positive experiences) was observed to exert a mediating effect on the relationship between PSS and LS.
Similarly, as given in Figure 2b, the total effect (β = 0.334, P < 0.01) from PSS to LS was at a significant level (Step 1). Moreover, the direct path from PSS to Negative experiences (β = −0.251, P < 0.01) was significant (Step 2). Meanwhile, path from the mediator, namely, Negative affect (β = −0.357, P < 0.01) to LS was significant (Step 3). Even after inserting mediator in model, the direct path from PSS to LS remained significant (β = 0.241, P < 0.01) (Step 4). Moreover, the mediating variable (positive experiences) was observed to exert a partially mediating effect on the relationship between PSS and LS.
DISCUSSION
The overarching goal of the current study was to examine how cancer patients generate pathways to LS. Given this goal, the current study sought to answer the following questions. (a) Does significant relationship exist between self-reports of PSS and facets of SWB (affective experiences and LS). (b) Does significant relationship exist between different facets of SWB (Affective experiences and LS). (c) Does positive and negative emotional experiences mediate the relationship between PSS and LS?
Bivariate correlations were analyzed to determine the relationships between PSS, affective experiences and LS. The results revealed significant positive relationship between PSS and LS. These results suggest that cancer patients who report more social support are more likely to have satisfaction with their life. This result is consistent with previous findings[35] and supporting first hypothesis of the present study. To explain this finding, it must be said that those people who perceive receiving high social support evaluate themselves as competent and successful in terms of interpersonal relations.[36] These evaluations have effects on the emergence of positive evaluations of life in people. In addition, perceived support may increase one's coping competence by providing comfort that supports are available if needed. Certain psychological characteristics like optimism, future orientation and perceived control, promote and maintain overall satisfaction with life.[37]
The relationship between PSS and Positive and Negative emotional experiences clearly showed that PSS was highly correlated with positive experiences (r = 0.598, P < 0.01). However, negative experiences (r = −0.420, P <.01) were inversely related to PSS. These findings favored second and third hypothesis. Previous research also reveals that positive affect has positive relationship with social support[3839] and a negative relation with stress.[40] Meanwhile, negative affect has a negative relationship with social support.[1741] Studies examining the facets of social support evidenced that positive affect was predicted by family embeddedness and provided support, while the decreased negative affect was predicted by perceived support.[13]
Findings of the mediation analysis indicated that PSS not only have direct effects on LS but also indirect effects that are mediated by positive and negative affective experiences. These results provide compelling support for the mediation hypothesis indicating that perception of support received by cancer patients during and after treatment is important in explaining LS of patients. Furthermore, beneficial effects stem from an increased level of positive feelings.
More specifically, positive emotional experiences fully mediated the relationship between PSS and LS. Further, negative emotional experiences partially mediated this relationship. From these findings we speculate that breast cancer patients perceive high support from their spouse, family, friends, and surroundings when they experience positive feelings from social relations. In other words, positive feelings serve as a catalyst to enhance LS of cancer patients. The findings of this study share some similarities with studies of.[4243] The results are also in line with positive psychological theory which emphasizes the importance of examining how positive psychological variables (e.g. resilience, positive affect, interpersonal connectedness) may serve to preserve and promote mental health and positive psychological outcomes.[44] However, negative affect being related to neuroticism[1945] and the tendency of individuals with negative affect to be introverted may lead these individuals to be less involved in social interactions, and in turn, let them perceive less social support. It could also be said that patients with high negative feelings may perceive social support less due to a more limited interaction compared to normal healthy individuals. This condition may reflect negatively on LS decreasing function of PSS. For example, Çivitci[46] posited that negative affect has a buffer role against the stress decreasing function of social support.
As a result, it can be understood from the findings of the present study that the relation between social support and LS is more susceptible to positive affect, and with the increase in positive affect the complementary function of social support for LS increases. The current study is significantly important in revealing the limitation of the complementary function of social support. Moreover, in the case of intense experiences of negative feelings by breast cancer patients such as anxiety depression and loneliness the insufficiency of social support indicates that the patient needs psychological care also. When social support is perceived insufficient, preventive and intervening studies counselling and guidance centres, as well as psychological consultations, may help for necessary support.
In summary, this study extended insights into the complex interactions among social support, affective experiences and LS of Indian breast cancer patients. The important path from perceived support to affect to LS determines the internal mechanism between social support and LS. The results of the current study can provide valuable guidance in implementing psychological interventions to improve LS and other psychological functioning of cancer patients. Improving perceived support among cancer patients can be used as a complementary therapy to help such people to improve their LS. It can also be used as an active therapy to help them manipulate the impact of affective balance to improve their LS.
However, the current study has several limitations. First, the data in this study were collected only through self-report measures, which could be a threat to internal validity. To reduce the impact of subjectivity, multiple assessment methods should be used for assessment. Second, the cross-sectional design of this study does not make cause-effect inferences. Future research may test the mediation model of using longitudinal or experimental studies. Third, the results of the current research are based on the 2D measure of affect balance. In future studies, PSS must be examined in different facets. Other possible mediating factors, such as loneliness, self-esteem and happiness, must also be explored. Finally, the sample in the current study was obtained from the population of breast cancer. Thus, whether the current findings can be generalized to other cancer population groups as well as other life-threatening disease population groups requires further investigation.
Clinical implications
It is well known that cancer causes both physical and psychological harm. In this age of evidence based practice, the present study provides a scope for the scientific evaluation of the association among affective balance, PSS and satisfaction with life among cancer patients. This study has significant clinical implications for palliative care practice. It will not only contribute toward the theoretical understanding of psychological side of cancer but will also help health care professionals addressing emotional experiences and social support network as coping strategies along with medical treatment to improve psychological functioning and thus mental health. While preparing psychological intervention modules for cancer patients, ability of patients to manage their emotions should not be ignored while focusing on social support to reduce distress symptoms. Targeted additional and personalized interventions should be used as an effective strategy for long term improvement in health-promoting behavior.
CONCLUSION
The current study provides an empirical framework for the researchers through testing the mediating effects of affective experiences between social support and LS in a sample of Indian breast cancer patients. In consideration of the probable mechanisms, it can be stated that the study has an interesting premise that the proximal cause of LS is not the direct effect of PSS but instead that PSS causes positive affect to exceed negative affect, which then causes LS to increase. These findings may help to design effective psychological interventions aimed at improving social support and affective balance in cancer patients. Attitudes such as involving the partner and the family in treatment, so they become aware of the problems women with breast cancer face, educating women concerning the importance of social support, teaching them to ask for help and discuss their needs, are exercises of social support.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Social attachments, group structures, and health behavior. Handbook of Health Behaviour Research. 1997;1:268-89.
- [Google Scholar]
- Social Support Measurement and Intervention: A Guide for Health and Social Scientists. 2000
- [Google Scholar]
- The theory of planned behaviour and healthy eating: Examining additive and moderating effects of social influence variables. Psychol Health. 2000;14:991-1006.
- [Google Scholar]
- Beyond the hedonic treadmill: Revising the adaptation theory of well-being. Am Psychol. 2006;61:305-14.
- [Google Scholar]
- Know thyself and become what you are: A eudaimonic approach to psychological well-being. J Happiness Stud. 2008;9:13-39.
- [Google Scholar]
- Understanding the links between social support and physical health: A lifespan perspective with emphasis on the separability of perceived and received support. Perspect Psychol Sci. 2009;4:236-55.
- [Google Scholar]
- The relationship between social support and physiological processes: A review with emphasis on underlying mechanisms and implications for health. Psychol Bulletin. 1996;119:488-531.
- [Google Scholar]
- Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J Personal Soc Psychol. 1989;57:1069-81.
- [Google Scholar]
- Subjective well-being: Three decades of progress. Psychol Bulletin. 1999;125:276-302.
- [Google Scholar]
- Pursuing happiness: The architecture of sustainable change. Rev General Psychol. 2005;9:111-31.
- [Google Scholar]
- The relationship between social support and subjective well-being across age. Soc Indic Res. 2014;117:561-76.
- [Google Scholar]
- Close personal relationships and health outcomes: A key to the role of social support. Handbook of Personal Relationships. 1997;2:547-73.
- [Google Scholar]
- Social support as a mediator in the relation between functional status and quality of life in older adults. Psychol Aging. 1996;11:34-44.
- [Google Scholar]
- Friends and family: A cross-cultural investigation of social support and subjective well-being among college students. J Posit Psychol. 2013;8:65-75.
- [Google Scholar]
- Diferences in how trait emotional intelligence predicts life satisfaction: The role of affect balance versus social support in India and Germany. J Happiness Stud. 2013;14:51-66.
- [Google Scholar]
- Development and validation of brief measures of positive and negative affect: The PANAS scales. J Personal Soc Psychol. 1988;54:1063-70.
- [Google Scholar]
- Social support and affect balance mediate the association between forgiveness and life satisfaction. Soc Indicat Res. 2015;124:671-68.
- [Google Scholar]
- Current status of breast cancer management in India. Indian J Surg 2020 DOI:10.1007/s12262-020-02388-4
- [Google Scholar]
- Psychosocial disorders in women undergoing postoperative radiation and chemotherapy for breast cancer in India. Indian J Cancer. 2010;47:296-303.
- [Google Scholar]
- Social support and achievement motivation among adolescents. Int J Humanities Arts Med Sci. 2015;3:117-24.
- [Google Scholar]
- Social support, social dysfunction and stressful life events in neurotic patients. Indian J Psychiatry. 1996;38:23-9.
- [Google Scholar]
- Social support and treatment outcome in alcohol dependence syndrome in armed forces. J Clin Diagnostic Res. 2015;9:1-5.
- [Google Scholar]
- Perceived social support and re-admission: A comparative study in re- admitted and non-admitted persons with schizophrenia. Global Res Analysis. 2013;2:194-6.
- [Google Scholar]
- Life events, social support, coping strategies, and quality of life in attempted suicide: A case-control study. Indian J Psychiatry. 2013;55:46-51.
- [Google Scholar]
- New well being measures: short scales to assess flourishing and positive and negative feelings. Soc Indic Res. 2010;97:143.
- [Google Scholar]
- Validating the flourishing scale and the scale of positive and negative experience in India. Mental Health, Religion & Culture. 2016;19:943-54.
- [Google Scholar]
- The affective and cognitive context of self-reported measures of subjective well-being. Soc Indic Res. 1993;28:1-20.
- [Google Scholar]
- Standardization and validation of Hindi version of satisfaction with life scale. Indian J Psychol Educ. 2020;10:106-11.
- [Google Scholar]
- SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36:717-31.
- [Google Scholar]
- Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychol Methods. 2002;7:422.
- [Google Scholar]
- Effect of perceived social support on life satisfaction of university students. Europ Cancer Res. 2013;1:1083-94.
- [Google Scholar]
- Attachment, social competencies, social support, and psychological distress. J Counselling Psychol. 2005;52:358-67.
- [Google Scholar]
- Positive affect, negative affect stress and social support as mediators of the forgiveness health relationship. J Soc Psychol. 2012;152:288-307.
- [Google Scholar]
- Links between stress, positive and negative affect and life satisfaction among teachers in special education schools. J Happiness Stud. 2013;14:731-51.
- [Google Scholar]
- Anxiety affect self esteem and stress: Mediation and moderation effects on depression. Plos One. 2013;8:E73265.
- [Google Scholar]
- Functions of social support and self verification in association with loneliness, depression and stress. J Health Communication. 2014;19:82-99.
- [Google Scholar]
- Happiness unpacked: Positive emotions increase life satisfaction by building resilience. Emotion. 2009;9:361-8.
- [Google Scholar]
- Positive emotions, hope, and life satisfaction in Chinese adults: A test of the broaden-and-build model in accounting for subjective well-being in Chinese college students. J Posit Psychol. 2019;14:829-35.
- [Google Scholar]
- Positive affect, negative affect and social interaction. J Personal Soc Psychol. 1996;71:796-809.
- [Google Scholar]
- The moderating role of positive and negative affect on the relationship between perceived social support and stress among college students. Educ Sci. 2015;15:565-73.
- [Google Scholar]




