
Translate this page into:
Return to Work in Cancer Patients: A Systematic Review and Meta-analysis
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Diseases and accidents bring about the disorder at someone's job insofar as one is not able to return to her/his previous work. These cases are related to the amount of occurred accidents, type of disease, and one's job.
Aim:
The aim of this study was to evaluate the factors that affect return to work (RTW) in cancer survivors using a systematic review and meta-analysis design.
Methods:
This is a systematic review and meta-analysis study. We searched the PubMed, Scopus, SID, Google, Elsevier, Google Scholar and Web of Science databases using following keywords: Return to work, cancer patients, employment status, cancer survivors from 2002 to 2017. The rate of return to work in cancer patients based on age group and risk factors was calculated using subgroup analysis. Data were analyzed using STATA software (version 11.1).
Results:
The total sample size was 4675 people with a mean of 668 in each study. The frequency of studies in the world consists mainly of five studies (71.5%) from Europe continent (the Netherlands and Denmark) and two studies (28.5%) from Asia continent (Iran and Japan). The overall rate of RTW estimated at 72% (68%–77%). The percentage of RTW in Asia and Europe was 57% (50%–65%) and 52% (43%–60%), respectively. Surgery had the highest percentage of treatment options in patients with cancer with 46% (25%–68%), followed by radiotherapy and chemotherapy with 37% (29%–46%) and 36% (23%–49%), respectively. Breast cancer and gastrointestinal cancer were the most and less common type of cancers with 36% (19%–54%) and 16% (7%–26%), respectively.
Conclusion:
The overall rate of RTW estimated at 57%. Nonetheless, the faster diagnosis and regular screening could improve the survival rate of cancer patients and the increase of RTW.
Keywords
Cancer patients
cancer survivors
employment status
meta-analysis
return to work

INTRODUCTION
Diseases and accidents result in the problem at someone's job insofar as one is not able to return to her/his previous work. The extent of this problem is related to the accident rate, type of disease, and one's job.[12] Given the development of societies and technology and new equipment in medical science, it is possible to provide a condition that one can return to the workplace after a period of treatment.[34] Diseases that exclude one from work divided into trauma disease and internal disease.[56] Cancer is one of the main diseases which impair one's normal life with many patients having to temporarily leave their job during treatment. In some extreme cases, they are forced to leave the job permanently.[78] Individuals who are not able to return to their workplace impose a burden on their families and society.[9] Regardless, the monetary costs associated with loss of work due to disease, it also has some negative psychological consequences in patients which in turn not only decrease the life expectancy and motivation in patients but also bring about anxiety in their families.[10] In most countries, one is insured after recruitment so that some of the deficits can be covered by insurance; even a salary will be determined to avoid any possible loss to the patients. For instance, in the Netherlands, patients can be benefited from the advantages of sick leave pay for 24 months.[211]
Recent advances in the diagnosis and treatment of cancer led to increasing number of cancer survivors.[12] Reintegration to society after treatment in cancer patients is an important purpose after initial treatments which can help many more patients to be able to return to work (RTW) and resume their normal life.[212] RTW after cancer treatment is a complex phenomenon which is influenced by many factors other than the disease itself.[9] There are several studies that reported the rate of RTWin cancer patients in the world. However, there are few studies regarding the comparison of RTW and its influencing factors in cancer patients in different parts of the world. Therefore, conducting a study using the meta-analysis methodology can provide the best evidence regarding the factors that affect cancer patients’ RTW. Such information is a necessity for health-care providers, decision maker, and other stakeholders to address this gap. The present study aimed to evaluate the factors that affect RTW in cancer survivors using a systematic review and meta-analysis design.
METHODS
This was a systematic review and meta-analysis. We searched the PubMed, Scopus, SID, Google, Elsevier, Google Scholar, and Web of Sciences databases using the following terms: Return to work, cancer patients, employment status, cancer survivors over a period of 10 years from 2007 to 2017.
Data extraction
First, the researcher collected all articles associated with RTW in cancer patients in the world and after the search a list of the abstracts prepared. Then, all articles with the searched terms in titles were included for initial assessment. Those articles that did not meet our criteria were excluded. In the next stage, a checklist of required information (researcher's name, article title, year, place, sample size, type of cancer, the number of women, the number of men, the percentage of RTW based on gender, place of study, cancer type, cancer stage, age groups, and type of job) was provided for the final assessment of all studies which had been initially assessed. Then, the final checklist was considered by researchers and related articles were included in the meta-analysis. About 40 articles were accessed using our keywords, of which 20 articles with related titles were included in the abstracts list of articles. The checklist for evaluating the quality of articles was filled by researchers for each study. Finally, the full text of seven articles was examined in the final analysis.
Statistical analysis
Given that in each article, the rate of RTW in cancer patients and the sample size was extracted, binominal distribution was used to calculate the variance in each study. The weighted average was used for a combination of the prevalence rates of various studies. Given weight at each article was according to the article's reverse variance. Random effects model was used in meta-analysis owing to the high difference in the prevalence rate in various studies and significant heterogeneity index. In this study, the rate heterogeneity was 89.6% which is classified as severe heterogeneity. Meta-regression was used in order to assess the relation of RTW in cancer patients by the year of study and the cause of the heterogeneity of studies’ results. The rate of RTW in cancer patients based on age group and risk factors were calculated using subgroup analysis. Data were analyzed using STATA software (version 11.1, (Stata Corporation, Texas, USA).
RESULTS
The search strategy identified 40 records. Of those, seven studies met the study inclusion criteria [Figure 1a]. Searches were performed from 2007 to 2017, and the total sample size was 4675 people with the mean of 668 patients per study. Of seven studies that were selected, five studies (71.5%) had been done in Europe continent (the Netherlands and Denmark) and two studies (28.5%) from Asia continent (Iran and Japan).
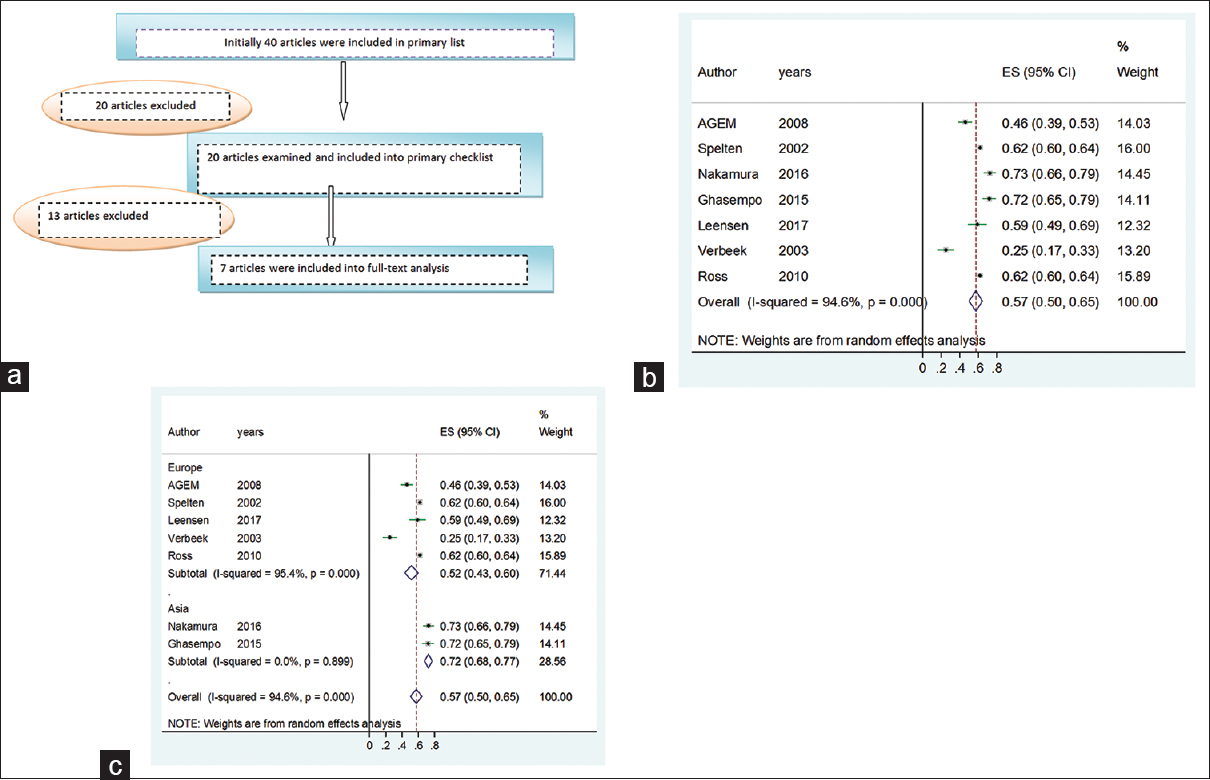
- (a) Flowchart of search strategy and number of included studies. (b) Forest plot of the overall rate of return to work with 95% confidence interval for all studies (overall and separately) based on the random-effects model. Line segments show confidence interval of the overall percentage of return to work. The midpoint of each line segment shows an estimated overall rate of return to work in each study. Diamond sign shows the confidence interval of the total rate of return to work for all studies. (c) Forest plot of the overall rate of return to work according to the continent with 95% confidence interval for all studies generally and separately based on the random-effects model. Line segments show confidence interval of the overall percentage of return to work according to the continent where the study has been conducted. The midpoint of each line segment shows an estimation of the overall rate of return to work pursuant to the continent in each study. Diamond sign shows the confidence interval of the overall rate of return to work pursuant to the continent for all studies
The highest percentage of RTW in cancer patients was in Nakmura et al. study, in Japan, with 73%[3] and the lowest percentage was related to Verbeek et al. study, in the Netherlands with 25%.[6] Articles characteristics are shown in Table 1.
| Authors | Country | Year | Sample size | Male (n) | Female (n) | Mean of age | SD of age | RTW (%) |
|---|---|---|---|---|---|---|---|---|
| de Boer et al.[1]* | The Netherlands | 2008 | 195 | 117 | 78 | 42.2 | 9.3 | 46 |
| Spelten et al.[2] | The Netherlands | 2002 | 2433 | 1403 | 1030 | 28.5 | 6.7 | 62 |
| Nakamura et al.[3] | Japan | 2016 | 199 | 47.0 | 9.7 | 72 | ||
| Ghasempour et al.[4] | Iran | 2015 | 165 | 63 | 102 | 43.83 | 10.49 | 72 |
| Leensen et al.[5] | The Netherlands | 2017 | 93 | 84 | 9 | 47.9 | 7.4 | 59 |
| Verbeek et al.[6] | The Netherlands | 2003 | 100 | 67 | 33 | 42.0 | 8.6 | 25 |
| Ross et al.[7] | Denmark | 2012 | 1490 | 952 | 538 | 45.5 | 8.9 | 62 |
*Numbers indicate reference number. SD: Standard deviation, RTW: Return to work
Table 2 shows the quality of the articles which apprised using checklist consists of seven criteria. Based on those criteria, articles were divided into three different quality including favorable quality (score 7), average quality (score 5–6), and weak quality (score below 5). Ultimately, seven articles were assessed, three articles with high quality, and four articles with average quality.
| Authors | Country | Year | Sample size | Male (n) | Female (n) | RTW (%) | Mean of age | Type of cancer | Type of treatment | Total score |
|---|---|---|---|---|---|---|---|---|---|---|
| de Boer et al.[1]* | The Netherlands | 2008 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 7 |
| Spelten et al.[2] | The Netherlands | 2002 | ✓ | ✓ | ✓ | ✓ | ✓ | - | - | 5 |
| Nakamura et al.[3] | Japan | 2016 | ✓ | - | - | ✓ | ✓ | ✓ | ✓ | 5 |
| Ghasempour et al.[4] | Iran | 2015 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | - | 6 |
| Leensen et al.[5] | The Netherlands | 2017 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | - | 6 |
| Verbeek et al.[6] | The Netherlands | 2003 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 7 |
| Ross et al.[7] | Denmark | 2012 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 7 |
*Numbers indicate reference number. RTW: Return to work
Given the heterogeneity in articles (I2 index, 64.6%), the confidence interval for each study and all the studies were based on the random effects model.
Figure 1b shows the overall rate of RTW which was 57% (50%–65%). Figure 1c shows the overall rate of RTW based on the continents which were 72% (68%–77%) and 52% (43%–60%) in Asia and Europe, respectively. The high I2 index showed that the results of studies were strongly different and the low I2 index showed the results of the studies were strongly similar.
Figure 2a-c (Forest plot) shows treatment methods for cancer patients in which the highest percentage was related to surgery 46% (25%–68%) and radiotherapy and chemotherapy were next with 37% (29%–46%), and 36% (23%–49%), respectively.

- (a) Forest plot of the effectiveness rate of surgery in cancer patients with 95% confidence interval for all studies (generally and separately) based on the random-effects model. Line segments show confidence interval of the effectiveness rate of surgery in patients with cancer in each study. The midpoint of each line segment shows the estimation rate of chemotherapy treatment effectiveness in each study. Diamonds sign shows the confidence interval of effective chemotherapy treatment in cancer patients for all studies. (b) Forest plot of the effectiveness rate of chemotherapy in cancer patients with 95% confidence interval for all studies (generally and separately) based on the random-effects model. Line segments show confidence interval of the effectiveness rate of chemotherapy in patients with cancer in each study. The midpoint of each line segment shows the estimation rate of chemotherapy treatment effectiveness in each study. Diamonds sign shows the confidence interval of effective chemotherapy treatment in cancer patients for all studies. (c) Forest plot of the effectiveness rate of radiotherapy in cancer patients with 95% confidence interval for all studies (generally and separately) based on the random-effects model. Line segments show confidence interval of the effectiveness rate of radiotherapy in patients with cancer in each study. The midpoint of each line segment shows the estimation rate of chemotherapy treatment effectiveness in each study. Diamonds sign shows the confidence interval of effective chemotherapy treatment in cancer patients for all studies
Figure 3a-e (Forest plot) shows the percentage of various cancers separately, which breast cancer had the highest percentage with 36% (19%–54%), followed by genital cancer, leukemia, and other cancer with 31% (11%-51%), 26% (14%-39%) and 24% (10%-39%), respectively. Gastrointestinal cancer had the lowest percentage of 16% (0.7%–26%).

- (a) The rate of breast cancer with 95% confidence interval for all studies (overall and separately) based on the random-effects model. Line segments show confidence interval of the rate of breast cancer in each study. The midpoint of each line segment shows the estimation rate of breast cancer in each study. Diamond sign shows the confidence interval of the rate of breast cancer for all studies. (b) The rate of leukemia with 95% confidence interval for all studies (overall and separately) based on the random-effects model. Line segments show confidence interval of the rate of leukemia in each study. The midpoint of each line segment shows the estimation rate of leukemia in each study. Diamond sign shows the confidence interval of the rate of leukemia for all studies. (c) The rate of genital cancer with 95% confidence interval for all studies (overall and separately) based on the random-effects model. Line segments show confidence interval of the rate of genital cancer in each study. The midpoint of each line segment shows the estimation rate of genital cancer in each study. Diamond sign shows the confidence interval of the rate of genital cancer for all studies. (d) The rate of gastrointestinal cancer with 95% confidence interval for all studies (overall and separately) based on the random-effects model. Line segments show confidence interval of the rate of gastrointestinal cancer in each study. The midpoint of each line segment shows the estimation rate of gastrointestinal cancer in each study. Diamond sign shows the confidence interval of the rate of gastrointestinal cancer for all studies. (e) The rate of other cancers with 95% confidence interval for all studies (generally and separately) based on the random-effects model. Line segments show confidence interval of the rate of other cancers in each study. The midpoint of each line segment shows the estimation rate of other cancers in each study. Diamond sign shows the confidence interval of the rate of other cancers for all studies
The overall rate of RTW based on the study sample size showed in Figure 4. As shown in Figure 4, the studies which had more sample size, the rate of RTW was higher.
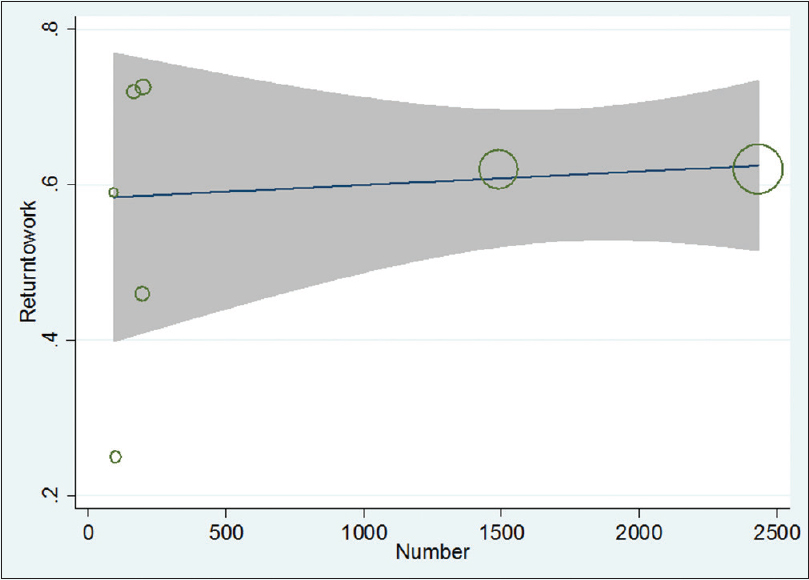
- The overall rate of return to work based on the study sample size
The studies’ meta-regression was according to the association between by the year of study and the overall rate of RTW and showed the overall rate of RTW was higher in newer studies than the older ones [Figure 5].

- Studies meta-regression based on the association between the year of study and the rate of return to work
Funnel plot in figure 6 shows no indication of publication bias. It is shows in funnel plot symmetrically. Circles’ size shows the weight of studies (bigger circles shows more sample and smaller circles shows fewer sample).
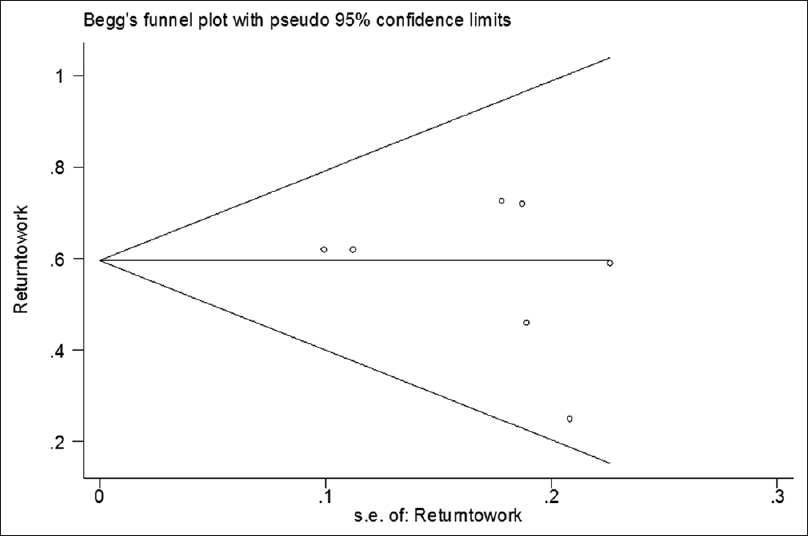
- Funnel plot of publication bias. It is shown in Funnel plot symmetrically. Circles’ size shows the weight of studies (bigger circles show more sample and smaller circles show fewer sample)
DISCUSSION
This meta-analysis and systematic review aimed to provide the information for the health-care providers and policy-makers to facilitate cancer patients RTW after the treatment.
Given the results, the overall rate of RTW was 57% (50%–60%). While in some other studies, the rate of resuming work in cancer survivors was between 25% and 73%.[36] This difference was owing to cancer and treatment's type among the patients. In some studies, the overall rate of RTW estimated at between 46% and 62%[1245] which shows the rate of RTW in cancer patients would be admissible if treatment be done timely.
In consonance with the results, the overall rate of RTW was calculated based on continents which the rate of RTW in Asian studies was higher than European studies. This disparity can be attributed to the European studies being older than Asian studies. Another point that arises is the difference in cancer type, treatment type, and society.
According to our findings, the surgery was the most common type of cancer treatment followed by radiotherapy and chemotherapy. Although, usually a combination of these therapies are used in various stages of cancer treatment, none of the studies. However, none of the studies include a report on the relationship between the type of treatment and patient RTW. Hence, we could not identify such a relationship.
According to the results of this study, breast cancer was the common type of cancer, followed by genital cancer, leukemia, and other cancers, respectively.
One hypothesis is that gender can be considered as a risk factor in cancer survivors in terms of RTW. In none of the studies in this review, the difference of RTW was reported by breakdown of gender. However, the previous studies showed a significant difference between sickness absence pursuant to gender regardless of type and the degree of disease progression. Further studies are required to examine the association between the rate of return to work and cancer survivors’ gender.
The study findings also showed that the rate of RTW was more in studies with more sample size and it rose with the increase of sample size.[1234567] The reason can be attributed to age, gender, job type, genetic, and heredity causes[1234567] which are suggested these cases, be considered in the future studies.
According to the results, the rate of RTW was higher in newer studies.[67] It may be due to recent advances in cancer treatments, and faster and more accurate diagnosis.
Interventions which improve the rate of RTW in cancer patients should be developed. Creating job opportunity according to the patient status should be provided since it is not possible for all the patients to return to their previous job or they would not be qualified for it anymore. Providing insurance for refractory diseases such as cancer which can cover-up sick leave pay to patients for 2 years is effective in reducing patients and their families’ stress and anxiety.
Limitations
This study had several limitations. First, in most of the selected studies, participants were not selected randomly, which limit the generalization of the study findings to the total population of cancer patients. Furthermore, the number of examined variables and their relationship with RTW was limited in some of the selected studies.
This study had some limitations. The rate of RTW was not determined based on cancer's degree and type and by breakdown of treatment type. The rate of RTW was not stated according to the gender and cancer patients’ age group and stated generally. Moreover, follow-up after treatment was not performed in studies and was not specified whether RTW was considered on a temporary basis, or the patient has left his/her job due to treatment again.
CONCLUSION
This study revealed somewhat the effective factors on RTW in cancer patients. The awareness of health-care providers and employers of these factors can be effective so as to diagnosing of cancer patients’ problems and providing more support for those patients. In this study, the estimated rate of RTW was 57%. Considering the advancements made in cancer diagnosis and treatment over the recent decade, it is expected that more cancer patients will be able to return to their work in the future. Therefore, the planning about job prospect of the patients should be considered as a part of the process of treatment and the rehabilitation of the patients.
Financial support and sponsorship
We would like to thank the Deputy of Research and Technology, Ilam University of Medical Science for approving and funding this research.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to thank the Deputy of Research of Ilam University of Medical Science for approving and funding this research.
REFERENCES
- Factors reported to influence the return to work of cancer survivors: A literature review. Psychooncology. 2002;11:124-31.
- [Google Scholar]
- Return to work after cancer treatment of gynecologic cancer in Japan. BMC Cancer. 2016;16:558.
- [Google Scholar]
- Return to work and its relation to financial distress among Iranian cancer survivors. Asian Pac J Cancer Prev. 2015;16:2257-61.
- [Google Scholar]
- Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: A prospective study in the Netherlands. BMJ Open. 2017;7:e014746.
- [Google Scholar]
- Return to work of cancer survivors: A prospective cohort study into the quality of rehabilitation by occupational physicians. Occup Environ Med. 2003;60:352-7.
- [Google Scholar]
- Factors associated with danish cancer patients’ return to work. A report from the population-based study ‘the cancer patient's world’. Cancer Epidemiol. 2012;36:222-9.
- [Google Scholar]
- What work means to people with work disability: A scoping review. J Occup Rehabil. 2014;24:100-10.
- [Google Scholar]
- Qualitative meta-synthesis of survivors’ work experiences and the development of strategies to facilitate return to work. J Cancer Surviv. 2014;8:657-70.
- [Google Scholar]
- Early work patterns for gynaecological cancer survivors in the USA. Occup Med (Lond). 2012;62:23-8.
- [Google Scholar]
- Cross-national comparisons of sickness absence systems and statistics: Towards common indicators. Eur J Public Health. 2014;24:663-6.
- [Google Scholar]
- Cancer rehabilitation may improve function in survivors and decrease the economic burden of cancer to individuals and society. Work. 2013;46:455-72.
- [Google Scholar]




