
Translate this page into:
Purple Urine Bag Syndrome: A Scary but Easily Manageable Condition in a Patient with Prolonged indwelling Urinary Catheter
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
“Purple urine bag syndrome” (PUBS) is a rare but distressing presentation of urinary tract infection (UTI) among moribund patients on indwelling urinary catheter. A 56-year-old woman with carcinoma of the left breast and metastasis in vertebrae and liver was bed ridden. She was on Foley's catheter for 9 months, with the last catheter changed 3 weeks back. A 75-year-old woman presented with non-Hodgkin's lymphoma for 2 years and moderately differentiated squamous cell carcinoma of the right parotid region (8 months). She experienced fall and fracture of femur, bed ridden, and on Foley's catheter for 7 years. She had facial wound with maggots for 3 days. Both the women developed purple-colored urine with no other symptoms of UTI. No investigations were carried out and they were empirically treated with nitrofurantoin, catheter change reassurance, and increased fluid intake. Urine color was normal by a week. PUBS can be managed easily at home with simple antibiotics, adequate hydration, and family/patient counseling in palliative care settings.
Keywords
Indwelling urinary catheter
palliative care
purple urine bag syndrome
urinary tract infection

INTRODUCTION
It is not uncommon to have bedridden patients on home-based palliative care. Bedridden patients on indwelling urinary catheters are at risk of urinary tract infection (UTI). One rare presentation of UTI could be sudden appearance of dark purple-colored urine in the catheter and urinary bag in otherwise asymptomatic patients. This condition, referred to as “purple urine bag syndrome” (PUBS), could be very scary and distressing to the patient and family. Management requires urine investigations including culture and sensitivity and treatment with suitable antibiotic/s. The condition is relatively rare and about 10-12 cases have been reported from India, mostly from intensive care setting. However, in our setting, many patients and families do not opt for detailed investigation and empirical treatment needs to be provided. Here we present report of PUBS in two women with advanced cancer, who were managed at home empirically.
CASE REPORT
A 56-year-old woman with carcinoma of the left breast (for 1 year) and metastasis in the vertebrae and liver was bedridden. Her pain was well controlled with oral tramadol and paracetamol. She had constipation and was on laxatives. She was on Foley's catheter for 9 months. The last catheter change was done 3 weeks back. The patient's daughter reported that the urinary bag was filled with purple-colored urine in the morning [Figure 1]. She had no other symptoms suggestive of UTI. The entire family was very much worried about this sudden change in urine color. They thought that it was due to cancer spreading to bladder and leading to some purple-colored discharge in the urine. The family refused bringing her to hospital for any further investigations or treatment. The family shared the pictures of urine bag and catheter on WhatsApp. She was hypertensive but not on any medications. A provisional diagnosis of PUBS was made and she was started on tablet nitrofurantoin 100 mg twice daily for 2 weeks. The family and the patient were counseled about the benign nature of the condition and the need to increase fluid intake. By 3rdday, the urine had become light colored [Figure 1] and was back to normal by end of the week. She expired after 4 months at home.
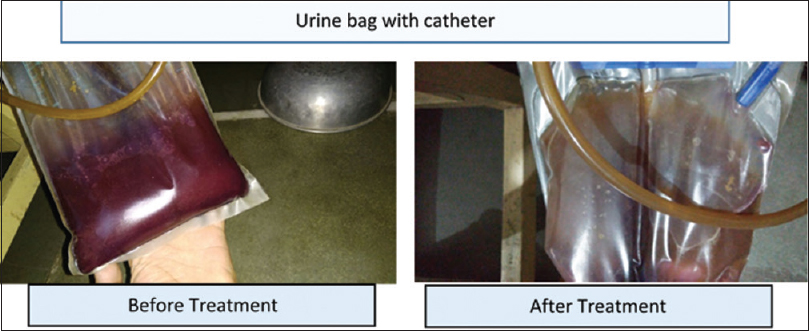
- Urine bag before and after treatment with antibiotics
A 75-year-old woman presented with non-Hodgkin's lymphoma for 2 years and moderately differentiated squamous cell carcinoma of the right parotid region (8 months). She had fall and fracture of the neck of the right femur for 7 years and was bedridden and on Foley's catheter. She experienced pain over the right side of the face (10/10) and maggots in the wound for 3 days. She was started on morphine, metoclopramide, bisacodyl, paracetamol, and pantoprazole. Three days later, she presented with purple-colored urine in the catheter and urinary bag. There were no other symptoms of UTI. The last catheter change was done 1 month back. She was started on tablet nitrofurantoin 100 mg twice daily for 2 weeks. The patient was counseled about the benign nature of the condition and the need to increase fluid intake. By 3rdday, the urine had become normal colored. She died 24 days later at home.
DISCUSSION
The first case of PUBS was reported in 1978.[1] However, historically, in 1812, King George III has been documented to develop bluish discoloration in his urine and the urinary catheter and bag.[2] King George III had chronic constipation which is believed to be an important risk factor for PUBS. It is a rare presentation of UTI. Its occurrence has been reported to be 8% to as high as 40% with long-term indwelling urinary catheter use.[345] The coloration is believed to be due to multiple bacterial UTI, most commonly Gram-negative bacteria. Providencia stuartii and Providencia rettgeri, Proteus mirabilis, Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, Morganella, and Citrobacter species, Enterococci, and Group B Streptococci are the commonly isolated bacteria. Purple coloration results due to a series of biochemical conversion reactions as shown in Figure 2.[678]
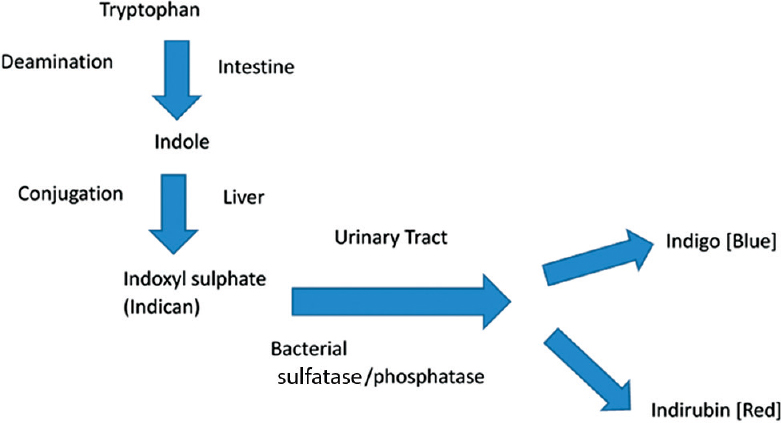
- Pathogenesis of purple urine bag syndrome
Chronically catheterized and constipated patients, especially women who have significant disability (limited ambulation) with the underlying comorbidities and cognitive impairment, are at the highest risk. Other risk factors include old age, alkaline pH of urine, institutionalization of the patients, and the use of plastic urinary catheter and bag.[56789]
Treatment is directed at the underlying UTI as well as control of constipation. Good urologic sanitation and change of catheter and antibiotics form the mainstay of treatment.[9101112] Good care of the urinary catheters will prevent UTIs and hence this phenomenon as well. PUBS is generally a benign process. Despite this fact, it is distressing for family, friends, and health-care workers who are unaware of this phenomenon and tend to become unusually alarmed because of the sudden inexplicable discoloration of the urine and sometimes the urine bag. Nevertheless, physicians should be aware of the fact that this syndrome signals the underlying recurrent UTIs, due to improper care of the urinary catheters and improper sanitation. PUBS is also associated generally with higher incidence of morbidity and mortality than UTIs alone without this occurrence.[910] PUBS has previously been considered a benign process in the majority of indwelling catheterized patients; however, with decreasing mortality over the last decade, early examination and aggressive antibiotic administration should be considered.[7] A recent meta-analysis has however shown that neither antibiotics nor catheter removal was associated with better outcomes.[11] Thus, a conservative approach with focus on simple antibiotics, adequate hydration, and family/patient counseling might be offered in palliative care settings.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
This case report was prepared while working on a Pallium India-supported project.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to acknowledge the financial and technical support provided by Pallium India, Thiruvananthapuram, for setting up palliative care services in our institution, which eventually led to developing this case report manuscript.
REFERENCES
- Purple urine bag syndrome in a dead-on-arrival patient: Case report and articles reviews. Am J Emerg Med. 2007;25:861.e5-6.
- [Google Scholar]
- Case analysis of purple urine-bag syndrome at a long-term care service in a community hospital. Chang Gung Med J. 2005;28:636-42.
- [Google Scholar]
- Purple urine bag syndrome: An alarming hue? A brief review of the literature. Int J Nephrol. 2011;2011:419213.
- [Google Scholar]
- Trends in the epidemiology of purple urine bag syndrome: A systematic review. Biomed Rep. 2018;8:249-56.
- [Google Scholar]
- Enzymatic degradation of urinary indoxyl sulfate by Providencia stuartii and Klebsiella pneumoniae causes the purple urine bag syndrome. J Clin Microbiol. 1988;26:2152-6.
- [Google Scholar]
- Purple urine bag syndrome: A systematic review with meta-analysis. Eur Geriatr Med. 2017;8:221-7.
- [Google Scholar]
- The purple urine bag syndrome: A visually striking side effect of a highly alkaline urinary tract infection. Can Urol Assoc J. 2011;5:233-4.
- [Google Scholar]




