
Translate this page into:
Caregivers’ Difficulty Rating Scale: Development and Initial Validation of a Tool to Identify the Unmet Needs of Indian Caregivers
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Caring for a cancer patient is debilitating for caregivers, especially among Indian population, as culturally people prefer to care at home than at nursing home. Unavailability of palliative care services and professional caregivers adds to the family burden.
Objectives:
Caregiving difficulties need assessment, but cancer-specific burden instruments are rare in the Indian context. This article presents development and initial validation of Caregiver's Difficulty Rating Scale (CDRS) and highlights the nature of caregiving burden on primary caregivers.
Methods:
A total of 108 items were prepared in English after case interviews and reviewing the existing scales for face validity. Experts judged the items for content validity, of which 54 items with 100% agreement were retained. Forward-backward policy was used for Hindi translation. Reliability analysis was performed with thirty respondents. The final scale was administered to 100 caregivers of head-and-neck cancer patients for internal consistency and item-scale statistics. For construct validity, know-group comparison was made using EORTCQOL instrument with caregiver-patients dyads.
Results:
High correlation among the three translated versions (r > 0.76, P < 0.01), Cronbach's alpha (0.948), and spilt-half coefficient (0.965) suggested translation reliability and scale consistency. Caregiver's burden had significant negative correlation with global quality of life of patients (−0.514**). Help for food arrangement, managing work–life, and treatment cost were the highly rated difficulties.
Conclusion:
CDRS had fifty items under four dimensions – physical, emotional, social, and financial. The scale requires further work on convergent and divergent validity and sensitivity to change which are underway. The study has implications for respite care. Community engagements and caregivers’ support group may work as sources of emotional and social support.
Keywords
Burden
cancer
caregiving
scale
validity

INTRODUCTION
Cancer affects not only the one who is surviving the disease, but also those caring for the patient. Cancer and its associated treatment place unexpected burden on the family. Caring for sick people, especially those with chronic and life-threatening disease, is a long, back-breaking, often unrewarding, and ultimately lonely affair. Cancer involves high caregiving demands and long-term dependencies that cause more strain to caregivers. In addition, it may hamper other routine activities such as work, leisure, and result in social isolation, financial strain, and deteriorating physical and mental health.[1] The caregivers are required to be around the patient both physically and psychologically almost the whole day which may give feelings of burden to caregivers that can diminish their quality of life (QOL). Impact of cancer on family caregivers is becoming an important subject of research, especially in the Indian context where people generally do not rely on paid caregivers, rather prefer to care for their sick relative themselves despite enormous difficulties. In light of this, it becomes essential to know-what is happening to the caregiver? What attributes does he/she bring to this experience? What is the impact of cancer diagnosis on caregiver and the entire family? What is the financial situation of the family? These and many more such questions have been explored for several decades and a complete picture of the many variables affecting caregivers and caregiving process is emerging. However, no attempts have been made to measure the different dimensions of burden. Further, literature supports the existence of burden inventories in the field of gerontology and mental health.[2] But, there is no specific burden scale which could have measured the caregiving burden on the caregivers of cancer patients. The need of the hour is to develop a systematic approach for assessing the degree of caregiving burden by quantifying the largely subjective domain of caregiving burden. The present research was undertaken with the main aim (1) to develop a scale to empirically measure the caregiving burden experienced by caregivers of cancer patients, (2) to report reliability and initial validation of the scale.
Ethical approval
This research was part of Doctoral Programme approved by the Department Research committee of Department of Social Work, DU, for which data collection was done at Rajiv Gandhi Cancer Hospital and Research Center, Delhi.
METHODS
The development and validation of this scale was done through the following five steps: (1) Conceptual definition of the construct and justification of the scale; (2) Developing preliminary pool of items; (3) Translation to the local language following the standard norms; (4) Reporting reliability and validity of the instrument; and (5) Development of scoring keys and norms.
Conceptual definition of the construct
A brief review of literature was conducted to identify varied dimensions being included in caregiving burden. Zarit and colleagues.[3] defined caregiving burden as the extent to which caregivers feel that their emotional or physical health, social life, and financial status are affected as a result of caring for their relatives. Given et al.[4] defined caregiving burden as alterations in caregivers’ emotional and physical health which can occur when care demands outweigh the available resources. George and Gwyther[5] defined caregiving burden as an all-encompassing term to describe physical, emotional, social, and financial toll of providing care. Thus, four major dimensions emerged from literature suggesting that caregiver's burden scale will have items spread over these four subscales, namely, physical health, emotional well-being, difficulties in social relationship, and financial concerns. The accumulative response on all the subscales will give comprehensive burden on caregivers.
Developing items
A scale is required to have moderately large number of items to measure a single construct. Further, items are so designed that they ask about the same theoretical construct but in a different way. A number of caregiver's burden inventories or related scales from the field of gerontology and mental health were reviewed for getting an idea of the content and language of the items. To begin with, 108 statements were prepared covering all the four dimensions of caregiving burden, i.e., physical, psychological, social, and financial concerns. Items were so worded as to respond on a 5-point Likert-type scale ranging from “Never” to “Always.” Individual-level open discussion with professionals such as doctors, nurses, counselors, and caregivers also guided the framing of items as this brought first-hand narration of difficulties experienced by caregivers. The following principles were upheld while framing the items:
-
Simple and straightforward items-questions were so designed that every respondent interprets it in the same way
-
Less instruction required to answer the items
-
Avoided double-barreled questions where the items actually combine two different questions into one
-
Avoided emotionally laden words or phrases
-
Reverse coding of few items under each dimension.
Validity procedure of the instrument
The validity of any measuring instrument depends on the accuracy with which it measures what it purports to measure when compared with a standard criterion. The British Psychological Society Steering Committee on Test Standard and Psychological Testing (1999)[6] says that “validity is concerned with what the test score actually measures.”
Literature presents several different types of validity all of which may not be determined by every scale, but it is important to ensure content and face validity as these two measures build a strong foundation for an empirical measure. Content and face validity involves qualitative procedure for item selection. Content validity is assessed by asking judges (experts on the topic) whether they agree that each item is about what is supposed to be about. Face validity is normally assessed by presenting judges’ finalized statements to the members of the target population (who will be completing the final measure). One or more of those who will be administering the test might also be asked.
Content validity
All the 108 statements were given to seven judges from different disciplines including one from medicine, one from nursing, two from psychology, two were psychiatric social workers, and another was a nongovernmental organization professional in cancer care. These statements were reviewed by the judges for their language, clarity, and validity to assess burden. Judges were also required to segregate the statements on different dimensions of burden (viz., physical, psychological, social, and financial).
Out of the 108 items, sixty items were retained as judges had 100% agreements on such items. On the basis of the remarks of the judges, items were then reworded for presenting clarity and avoiding ambiguity. This process dropped six items leaving 54 items in the scale.
Face validity
The 54 items as finalized by the judges were then pretested with five caregivers of cancer patients. The purpose here was not to score their response rather to understand what they felt while responding to these questions. Caregivers were qualitatively interviewed to share if items were easy to understand, present clarity, and if any emotional upsetting phrase was experienced. On the basis of their response, four more items were dropped as respondents found them either repeated, difficult to understand, or having scope to be merged with other items. Through this process, the final scale had fifty statements spread over four subscales. Each subscale also had 1/3rd reverse stated items so as to assess authenticity of the responses.
Process of deciding about the title of the scale
Judges were also requested to review different options for the title phrase, namely:
-
Caregiving Burden Inventory
-
Caregivers’ Burden Assessment Scale
-
Caregiver's Difficulty Rating Scale (CDRS).
Remarks from the judges conveyed that in the Indian context the term “burden” carries negative connotations. Since in the Indian culture, caring for the loved ones is considered as a responsibility, so nobody would be comfortable to accept the term “burden” as it may hurt sentiments of the target population. Therefore, it was suggested not to use the term “burden” in the title and substantiate the same with related term like “difficulty.” Thus, the “CDRS” was finalized as the title of the scale.
Translation of the scale
Initially, all the items were framed in English to make judges convenient at the initial stage as their contribution to work was paramount. Moreover, having two language versions of the scale would open avenues for reliability calculation. Further, Hindi translation was required to ensure cultural sensitivity of the scale as the majority of the population in North India where the scale was planned to be administered were friendly with Hindi. The standard policy of forth and back translation was used for translation of the scale in the following steps:
-
A panel of three judges consisting of one expert in Hindi, one expert in English to Hindi translation, and one layman who could give feedback on the simplicity of the words used
-
Hindi-translated scale was then reverse/back translated in English by a different panel of judges consisting of one expert in English, one expert in Hindi to English translation, and one layman who could give feedback on the simplicity of the words used.
Reliability of the translation
Reliability means consistency. A scale has reliability if repeated measurements under the same circumstances tend to produce the same results. In order to determine the reliability of the translated version, a sample of thirty persons from the general population was selected to avoid unnecessary trouble to the actual caregivers. This sample consisted of people in different capacities who could become caregiver at any stage in their life such as students, academicians, homemakers, working women, elderly, and professionals (doctor, psychologist, social worker, and engineer). The sample was first given the original English version to respond, the second time the Hindi version, and the third time the reverse English translation each after a gap of 1 week. The sequence of items in each version was jumbled in order to avoid directionality in responses. Since reliability is concerned with the degree of consistency or agreement between two independent sets of scores, they are expressed in terms of correlation coefficient. Here, correlation was calculated among the three versions of the scale which is presented in Table 1 for each subscale as well as the overall scale. Correlation coefficient among the three versions of all subscales as well for the overall scale [Table 1] was found to be significant, suggesting that translation is reliable and all the three versions convey the same meaning. Thus, the final Hindi version of the scale was ready to be tested in the actual setting.

Data collection and analysis
Data collection for reliability and validity testing was done with a sample of 100 head-and-neck cancer patient-caregivers dyads selected conveniently from one of the cancer care hospitals of Delhi namely RGCI & RC. In the absence of a cancer-specific caregiving burden scale in the Indian setting, criterion validity was out of question, so following COSMIN checklist,[7] know-group comparison was resorted for quantitative assessment of construct validity. For construct validity, know-group comparison was made using EORTC-QOL instruments and hypotheses were prepared on medical and demographic characteristics of caregiver-patients dyads. A sample of 100 head-and-neck cancer patients and their caregivers were recruited as dyads if they met the following criteria:
Inclusion criteria
-
A patient-caregiver dyad, wherein the patient has to be above 18 years of age and able to identify a primary caregiver
-
Patient with head-and-neck cancer, i.e., cancer that arises in the head or neck region (in the nasal cavity, sinuses, lips, mouth, salivary glands, throat, or larynx)
-
The patient must be getting active treatment for head-and-neck cancer from the cancer care institutions in Delhi for at least 6 weeks. During the 6 weeks’ treatment, the patient would get exposed to the side effects of treatment and caregivers will be escorting patient to the hospital frequently forcing a change in their daily routines. Patients with terminal disease were consciously excluded to avoid any emotional trauma and invasion to their time of togetherness.
Thus, N = n1 (100 patients) + n2 (100 corresponding caregivers) = 200 respondents.
A self-developed interview schedule was used for collecting demographic and medical data which were supplemented with patient's record file. Patients and their respective caregivers were interviewed separately to give them a comfortable zone for expressions.
Data were analyzed using SPSS software version 16 (SPSS Inc., IBM, USA) and using separate spreadsheets for reliability testing of translated versions as well as validity and reliability testing of the final scale. Item-scale analysis, Cronbach's alpha, and spilt-half reliability were performed to assess internal consistency of the instrument. For validity testing, known-group comparisons were made using EORTC-QOL questionnaire for patients and testing in accordance with caregiving burden. In addition, demographic and medical characteristics of the patients were also related with caregiving burden using appropriate statistical procedures.
RESULTS
A very large majority of patients (67%) were between 42 and 66 years of age, 23% below 42 and another 10% above 66 years of age. Cancer was mainly seen among males (88%) and females contributed to 12% of the total population. Nearly 53% of the patients were educated above secondary level. Cancer of oral cavity was most commonly reported, and the majority of diagnoses (66%) were made at advanced stage. Nearly 58% of the caregivers were younger than 44 years of age. Ratio of male-to-female caregivers was 1:1.4, meaning female caregivers outnumbered male by about 40%. Majority of the primary caregivers were spouse (55%); among them, females were in high majority (86%). Majority of caregivers (46%) had nuclear family, a majority of these families (60.86%) were small sized having 4–6 members. In more than 50% of the cases (53%), patient was the main earning member, while for another one-fourth proportion of the sample (25%), caregivers were the main earning member of the family. This suggests that cancer affected either patient's or caregiver's earning capacity, hampering the financial resources of the family.
In order to determine internal consistency of the scale and if each item is appropriate to be retained in the scale, Cronbach's alpha, spilt-half reliability, and item-scale analysis were performed using data from 100 caregivers. Cronbach's alpha is the most commonly used procedure of reliability. It is highly accurate and requires only a single application of the scale. A low alpha value suggests that some items either have very high variability or that the items are not measuring the same thing. Alpha should normally be at least 0.70 for reliability to be regarded as satisfactory.
Table 2 shows that the value of Cronbach's alpha for each subscale was significant enough to establish the internal consistency of the scale. The Cronbach's alpha of the overall scale for this sample was calculated as 0.948, with mean 137.6 and standard deviation of 39.429. Guttman's spilt-half coefficient for even and odd items was 0.965.

Item-scale analysis [Table 3] further showed that correlation coefficient of each item with their own subscale was significant for each item supporting item convergent validity except one item on keeping extra maid under financial subscale. Average of item-scale correlation for each subscale was above 0.6 except for financial subscale which was 0.5. A correlation value < 0.2 or 0.3 indicates that the corresponding item does not correlate very well with the scale overall and thus, it may be dropped.[89] Item analysis was further conducted to assess the suitability of deleting low value item from the scale. Cronbach's alpha if item deleted results are presented in Table 4 for financial sub-scale.


There is not much difference in Cronbach's alpha (0.763–0.795) of the financial scale if item with low item correlation (i.e., hiring of extra maid) is deleted [Table 4]. Further, item-analysis must be guided not only by empirical (operational) procedures, but also by theory-driven (validity) considerations, as judges voted for 100% agreement for retention of items. So, at this stage, item was retained, but will be given high consideration for further statistical operations at the next phase of this work.
In the absence of a standard caregiving scale specifically for caregivers of cancer patients, known-group comparison approach was used for convergent validity of the scale. Caregiving burden was also compared with QOL of the patients. The correlation coefficient was calculated among all the five dimensions of QOL (physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning) and all the four dimensions of caregiving burden (viz., physical, psychological, social, and financial) as well as the total scale as a whole [Table 5].

Caregiving burden presented significant negative correlation with the global quality of life of patients (−0.514**), as well as their physical (−0.43**), role (−0.42**), emotional (−0.45**), cognitive (−0.38**), and social functioning (−0.48**). Subscales of caregiving burden had significant negative correlation with physical, emotional, role, cognitive, and social functioning except financial burden experienced by the caregivers which had significant negative correlation only with emotional and social functioning of patients. Caregiving burden was further found to have significant positive correlation with fatigue, pain, insomnia, appetite loss, and financial difficulty subscales on EORTC [Table 6].

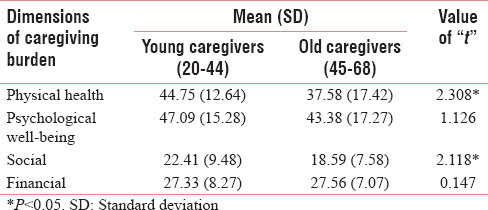
Thus, premise of the stress and coping model[10] states that, the greater the demand of patient's illness, more negative the consequences of the caregiving, which has been proved here. Other assumptions were drawn comparing caregiving burden with age of the patient, stage of their disease, as well as age of the caregivers following life span approach.[11] t-test for significance of mean [Table 7] between the young and old caregivers shows significant difference for physical (2.308*) and social (2.118*) dimensions of caregiving burden, suggesting that younger caregivers experience more physical as well as social burden than older caregivers.
Correlation coefficient was calculated between age of patients, stage of disease, and caregiving burden of the caregivers. Age was found to have significant negative correlation [Table 8] with caregivers’ psychological well-being (−0.212*) and social relationship (−0.240*), suggesting caregiving burden is high in case of young patients; however, assumption in case of stage of the disease was not significant.

DISCUSSION
This study presents an empirical tool to assess the caregiving burden of family members. The CDRS presents caregiving burden under four factors – (i) physical health which represents difficulties and disturbances experienced by caregivers in their day-to-day activities and their health; (ii) psychological well-being which represents emotional disturbances to the caregivers; (iii) social relationship which represents disturbances in caregivers’ social engagements and continuity of interaction in social circle; (iv) financial concerns which represent financial burden on family to meet the treatment cost and cutting short other expenses. A total of fifty items spread through the above four dimensions constitute the scale which can be used both in interview setting as well as self-report instrument. The average completion time for this scale is 15 min.
Although item-scale analysis presents high value of correlation, one of the items on “having special arrangement for food for the patient” did not have very high correlation value. This may be because in Delhi from where this sample is drawn, having maid and cook is quite common leaving less scope for caregivers to worry about this item. Similarly, item on role of counselor under psychological well-being did not have high correlation with scale suggesting that the role of counselors in cancer care has not yet been much recognized by patients and their families. Having this item on the scale gave scope to the caregivers to ask questions about counselor's role seeking help in the future. Item on employing extra maid or nurse under financial factor did not yield significant correlation with the total scale suggesting that this item could have been dropped from the scale. However, there was not much difference in Cronbach's alpha of financial subscale even if this item was deleted (0.763 with this item and 0.795 if item is removed). Retaining one item at this stage even with low significance can help develop a smaller version of scale at later stage and to valid the new version with the present longer version in the absence of enough scale on this subject. Since advantage of retaining this item was high over smaller statistical difference if deleted, it was decided to retain the same.
Internal consistency of a scale is important because it suggests how items are related with each other and how close are they to the theoretical construct. Cronbach's alpha and Guttman's split-half reliability coefficient were used to establish the internal consistency of the present scale. The Cronbach's alpha of the overall scale for this sample was calculated as 0.948 with mean of 137.6 and standard deviation of 39.429, while Guttman's spilt-half coefficient for even and odd items was 0.965, suggesting high internal consistency of the scale even if all the items are retained.
In the absence of a standard instrument to serve as reference scale to test the convergent validity, the present study resorted to known-group comparison. Theoretical model developed by Sales et al.[10] on stress and coping process of caregivers was used to identify quality of life of patients and their medical as well as demographics factors were related with care giving burden. Assuming that poor functioning status and high symptom burden of the patients give higher burden to the caregivers, scores of patients’ QOL as obtained by EORTC-QOL scale were compared with caregiving burden scores of the caregivers for known-group comparison. All the four dimensions of caregiving burden had significant negative correlation with global QOL of patients as well as their physical, emotional, role, cognitive, and social functioning except the financial burden experienced by the caregivers which had significant negative correlation only with emotional and social functioning. Thus, assumptions regarding the five dimensions of QOL and global QOL were satisfied with caregiving burden scale. Thus, premise of the stress and coping model between QOL of patients and caregiving experience of the caregivers has been satisfied by the present scale suggesting the validity of CDRS. Caregiving burden was correlated with QOL of patients in addition to comparison of caregiving burden with the age of patients and stage of their disease. Assumption was also drawn to correlate caregiving burden with age of the caregivers themselves.
Life span approach[11] emphasizes that the nature of problems and challenges associated with different age groups is not alike. Younger adults face major challenges of establishing their family including high income inflow and children are small who need to be looked after, cared for, and guided regularly. Hence, a hypothesis was proposed with respect to age of the caregiver keeping age 45 as the year of demarcation between young and old caregivers and the four dimensions of caregiving. t-test for significance of mean [Table 7] between the young and old caregivers shows significant difference for physical (2.308*) and social (2.118*) dimensions of caregiving burden, suggesting that younger caregivers experience more physical as well as social burden than older caregivers. Literature suggests that certain characteristics of the patient such as age, stage of disease, and the lower level of functioning of the patients (poor QOL) contribute to the greater caregiving burden.[12] Keeping same as the base, two-tailed assumption was drawn between age of the patient, stage of the disease, and caregiving burden. Correlation coefficient was calculated between age of the patients, stage of disease, and caregiving burden of the caregivers. Age of the patient showed significant negative correlation with caregivers’ psychological well-being and social relationship, suggesting that caregiving burden remains high for those caring for younger patients; however, assumption in case of stage of the disease was not significant suggesting that caregiving burden was independent of the stage of the disease.
CONCLUSION
The present study thus could satisfy a total of eight assumptions for known-group comparison, including five for QOL dimensions, one with global QOL, and one each for age of the patient and caregiver. Although this research could present a valid caregiving burden scale with satisfactory reliability and validity to be used specifically with family caregivers of cancer patients in the Indian setting, researchers need to use this scale with caution as this work has some inherent limitations too. First, convergent and divergent validity of the scale could not be well established yet due to unavailability of specific instruments in the Indian setting. Testing convergent-divergent validity using a smaller version of the scale as well as establishing responsiveness to change is in process. The scale has language barriers as it can be used only with Hindi- and English-speaking population. India being a multi-lingual country, this scale needs translation and adaption in regional languages too.
CDRS is a valid instrument designed to measure multidimensional difficulties experienced by caregivers of cancer patients. This scale can be used both in interview setting and as a self-report instrument. It is reliable and presents satisfactory validity, making it suitable for use in research and clinical settings.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- A new test of the construct validity of the CarerQol instrument: Measuring the impact of informal care giving. Qual Life Res. 2011;20:875-87.
- [Google Scholar]
- The Zarit Burden Interview: A new short version and screening version. Gerontologist. 2001;41:652-7.
- [Google Scholar]
- Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist. 1980;20:649-55.
- [Google Scholar]
- Burden and depression among caregivers of patients with cancer at the end of life. Oncol Nurs Forum. 2004;31:1105-17.
- [Google Scholar]
- Caregiver well-being: A multidimensional examination of family caregivers of demented adults. Gerontologist. 1986;26:253-9.
- [Google Scholar]
- The British Psychological Society. Psychological Testing UK. Available from: https://www.ptc.bps.org.uk/psychological-testing/getting-gripsour-terminology
- The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An International Delphi Study. Qual Life Res. 2010;19:539-49.
- [Google Scholar]
- The Cambridge Dictionary of Statistics. Cambridge: Cambridge University Press; 2002.
- Discovering Statistics Using IBM SPSS Statistics. New Delhi, India: Sage Publications; 2013.
- Predictors of strain in families of cancer patients. J Psychosocial Oncol. 1992;10:1-26.
- [Google Scholar]
- Developmental Psychology. New Delhi, India: Tata McGraw-Hill Education; 2001.
- Family Caregiving in Chronic Illness: Alzheimer's Disease, Cancer, Heart Disease, Mental Illness, and Stroke. Newbury Park: Sage Publications, Inc; 1991.




