
Translate this page into:
Perceived Barriers to Symptoms Management among Family Caregivers of Cancer Patients
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Caring for patients with advanced disease involves many concerns for caregivers. All aspects of health of the caregiver is compromised in the process of caring for the cancer patients. Usually, most of the terminally ill cancer patients live with their caregivers at home.
Objectives:
The aims of the present study was to identify the barriers to symptom management among caregivers of cancer patients and to find the association between perceived barriers to symptom management of caregivers' with their demographic variables and their patients' disease-related variables.
Materials and Methods:
A descriptive study was conducted among 768 family caregivers (FCGs) of cancer patients, and they were selected using convenient sampling technique. Data was collected from caregivers who were caring for their beloved one at least 2–3 h/day and who were above 20 years of age. Data was collected through a structured interview using barriers questionnaire and demographic pro forma after obtaining the consent from the caregivers.
Results:
The result shows that among 768 FCGs, 216 (28.1%) of them were in the age group between 31 and 40 years and most of them were spouses (45.6%). The perceived barriers of caregivers were less confidence on the management of symptoms. A total of 423 (55.1%) had lack of awareness about pain assessment and management of cancer by 681 (88.6%). Majority, i.e., 654 (85.1%) of them had financial problems in the family.
Conclusion:
FCGs take the major responsibilities both at the hospital and at home in caring for the cancer patients. Since FCGs had lack of knowledge on caring of cancer patients, there is a need for awareness program on the assessment and management of symptoms among cancer patients.
Keywords
Cancer
family caregivers
perceived barriers

INTRODUCTION
Family caregivers experience psychosocial distress while caring for cancer patients. Usually, terminally ill patients spend their end stages of life at home being cared for by their families, without formal homecare services.[1] The caregivers experience many barriers to manage the symptoms experienced by their beloved one who is suffering from cancers. Fear of addiction may be the main barrier to cancer pain management.[2] Depression among caregivers is mainly due to the fear of unemployment during caregiving, being the spouse of a patient, burden of caregiving, and disturbance of personal life.[3] Family caregivers (FCGs) experience many difficulties and have increased responsibilities during and after the treatment for cancer.[4] Caregiver's sleep disturbances contribute to depression, anger, and anxiety.[5] The struggle with symptoms and the decreased quality of life (QOL) continue for the cancer survivors and their caregivers throughout their survival.[6] FCGs experience and struggle with many issues in taking care of the cancer patients, especially in symptom management. Increasing the knowledge of caregivers is more important for symptom management among the cancer patients.[7]
Objectives of this study
The following objectives were:
-
To identify the perceived barriers to symptom management among the FCGs by using perceived barriers to symptom management tool
-
To find the association between perceived barriers to symptom management of caregivers' with their demographic variables and their patients' disease-related variables.
Hypothesis was tested at 0.05 level of significance
H1: There will be a significant association between perceived barriers to symptom management of caregivers with their selected demographic variables and their patients' disease-related variables such as age, education, income, type and stage of cancer, duration of illness, and duration of treatment.
MATERIALS AND METHODS
An exploratory survey was done among 768 FCGs of cancer patients who were closely related to the cancer patients (spouse, parents, children, or siblings) aged above 20 years and involved in patient care at least 2–3 h/day. Caregivers who were providing care to the cancer patients diagnosed to be in the 3rd or above stages of cancer of breast/cervix/head and neck/gastrointestinal tract (GIT)/lung/colorectal cancer and have undergone radiotherapy or chemotherapy or surgery or combination of them were included in the study. Twelve hospitals from the southern part of Karnataka (Manipal, Mangalore, and Bengaluru) were selected using purposive sampling. Of these 12 hospitals, seven hospitals have permitted to conduct the study. From 768 cancer patients, 768 FCGs (1:1) were selected using purposive method from the selected hospitals who fulfill the inclusive criteria. Data were collected using pretested structured interview tool after obtaining permission from the respective hospital administrators as well as consent from the caregivers. The description of the tools are given below.
Description of the tools
Tool 1: Demographic pro forma
This tool was developed to obtain the background information of the samples. The items included were age, gender, religion, marital status, education, occupation, family monthly income, and relationship to cancer patients.
Tool 2: Perceived barriers to symptom management
The tool consisted of 25 items. Each item score ranged from 0 to 4, i.e., “very much” carried a score of “4” and “not at all” carried “0.” Thus, the possible maximum score was “100,” and the minimum was “0.” Higher the score more are the perceived barriers. The reliability was established using Cronbach's alpha coefficient formula. The reliability coefficient obtained was r = 0.86.
Ethical considerations
The objectives of this study were informed to the FCGs, and informed consent was obtained. The study was approved by the Institutional Ethics Committee. Administrative permission was obtained from the seven reputed cancer hospitals who granted permission for data collection.
Statistical analysis
The obtained data were coded, tabulated, and analyzed using the SPSS package version 16 (IBM SPSS Inc., Chicago) and were interpreted using descriptive and inferential statistics on the basis of objectives and hypotheses of the study.
RESULTS
Out of 768 FCGs, 216 (28.1%) FCGs were in the age group between 31 and 40 years, the mean age of the FCGs of cancer patients was 41.63 ± 11.24 years and 454 (59.1%) were females. Majority, i.e., 678 (88.3%) of them were married, 225 (29.3%) of them had their education until primary school, and 374 (48.7%) of them were housewives [Table 1]. The data related to the relationship of caregivers with the cancer patients show that 350 (45.6%) of them were spouses [Figure 1].


- Caregivers relationship with cancer patients (n=768)
Description of perceived barriers to symptom management
This section presents the data of perceived barriers to symptom management while providing care to their beloved ones. For reporting frequency and percentage of perceived barriers to symptom management, frequencies of “a little bit” to “very much” were clubbed together for all the perceived barriers to symptom management. The frequency and percentage distribution of perceived barriers on symptom management among caregivers on all items are given in Tables 2a and b.

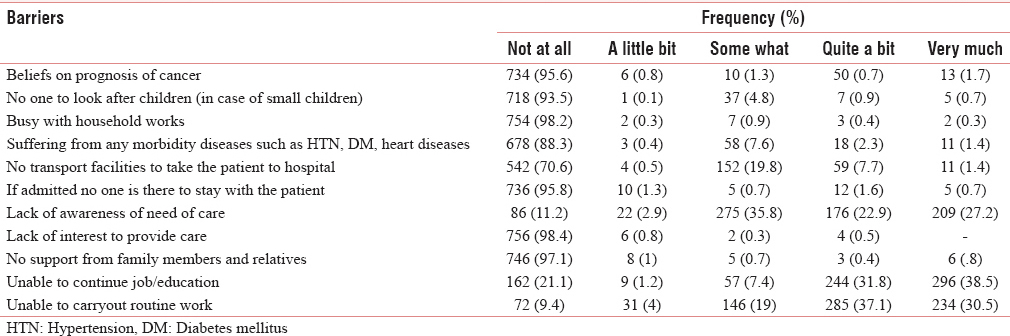
Out of 768 caregivers of cancer patients, most of them 423 (55.1%) had less confidence to manage symptoms, 681 (88.6%) had lack of awareness about pain assessment and management, and 666 (86.8%) of them had the inability to decide how and when to deliver the care. Majority, i.e., 654 (85.1%) of them had financial problems in the family, 750 (97.7%) had lack of knowledge about the disease, and 667 (86.9%) had lack of resources to provide care. Hence, FCGs need to be empowered on the management of cancer care. However, 96.9% (744) of the caregivers expressed that they do not have hesitation to administer the medication as prescribed by the doctors, 746 (97.1%) were willing to provide care, and 748 (97.4%) were not neglecting the cancer patients [Table 2a]. Majority of caregivers of cancer patients (88.8%) had lack of awareness of need of care, 606 (78.9%) had reported that due to hospitalization of patient caregivers could not continue their job/education, and 696 (90.6%) had reported that they were unable to carry out their routine work due to hospitalization of the patients. Seven hundred and eighteen (93.5%) of them perceived that there is no problem with regard to looking after their children, 754 (98.2%) did not have a problem with household work, and 736 (95.8%) had no problem to stay with the patient during hospitalization. Majority, i.e., 756 (98.4%) of them had interest in providing care and 746 (97.1%) had family support [Table 2b].
Association between caregivers' perceived barriers to symptom management with their demographic variables and their patients' disease-related variables
One-way ANOVA was computed to find the association between mean score of caregivers' perceived barriers to symptom management and their age, education, the income of the family and their patients' disease-related variables such as the type of cancer, duration of illness, duration of treatment and stage of cancer. Result shows in Table 3 that the association of caregivers education, income level, and type of cancer with perceived barriers to symptom management is statistically significant (F = 4.982, P < 0.001 and F = 9.101, P < 0.001 and F = 3.12, P < 0.015, respectively). Further, post hoc multiple comparison shows that education level increases with a decrease in perceived barriers (confidence interval [CI] =1.14–14.48, P = 0.003) and those who had income above Rs. 15,000 had lesser barriers than those who had income less than Rs. 2500/month (CI = 3.60–10.95, P = 0.001). Thus, it is interpreted that as the caregivers' educational status and income increases, the perceived barriers to symptom management decrease. FCGs perceived more barriers in caring the patients with cervical cancer when compared to cancer of GIT region (CI = 0.806, 7.75, P = 0.006).

DISCUSSION
It was found in the present study that majority, i.e., 681 (88.6%) of the FCGs had lack of awareness about pain assessment and management, 666 (86.8%) of them had inability to decide how and when to deliver the care, 750 (97.7%) had lack of knowledge about disease, and 70.3% reported that due to hospitalization of the patient the caregivers could not continue their routine education/work/job and nearly 725 (94.4%) of FCGs experienced financial burden due to the disease condition of the patients. These findings are supported by Valeberg et al., (2016)[2] who reported that concerns of both the patients and their FCGs about pain and the use of analgesics may act as barriers to effective pain management. Fear of addiction may be an important barrier to cancer pain management and the patients, and the FCGs need education about the perceived barriers to effective pain management. The financial burden was reported in studies conducted by Covinsky et al.,[8] Grunfeld et al.,[9] Deshields et al.,[10] Song et al.,[11] Yun et al.;[12] Tang;[13] de Córdova et al.,[14] on caregivers of cancer patients. Lukhmana et al.,[15] reported that majority of the caregivers were females (55%), the mean age was 40 years, and most of the caregivers were spouses (57.5%). Forty-three percent of caregivers missed work due to patient's illness, which ranged from missing work for a month (10%) to quit their job. Majority of the caregivers reported minimal burden (56.5%), and 37.5% of caregivers stated mild-to-moderate burden. Yakar and Pinar [16] in their study found that caregivers' life was affected negatively due to the caregiving responsibility and it affected their routine activities (53.3%). They also encountered problems in their work life (30%) and family relationship (15%). Financial problems were contributing factors on QOL. Turkoglu and Kilic,[17] seen in their study as caregiving adversely affects many aspects of the caregivers' life and recommended to train the caregivers to improve their QOL.
CONCLUSION
The result of this study emphasizes the importance of increasing the knowledge by education regarding the cancer symptoms management to the caregivers of cancer patients receiving homecare.
The caregivers experienced many barriers in providing care to their beloved ones, and there is a need to develop measures for effective management of symptoms and to improve QOL of the cancer patients and their caregivers.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank all the FCGs and all administrators of reputed cancer hospitals of Karnataka state for giving the permission to conduct the study.
REFERENCES
- Understanding economic and other burdens of terminal illness: The experience of patients and their caregivers. Ann Intern Med. 2000;132:451-9.
- [Google Scholar]
- Comparison of oncology patients' and their family caregivers' attitudes and concerns toward pain and pain management. Cancer Nurs. 2016;39:328-34.
- [Google Scholar]
- Prevalence and predictors of anxiety and depression among family caregivers of cancer patients: A nationwide survey of patient-family caregiver dyads in Korea. Support Care Cancer. 2013;21:2799-807.
- [Google Scholar]
- Review of the literature on the effects of caring for a patient with cancer. Psychooncology. 2010;19:1013-25.
- [Google Scholar]
- Distressing emotions in female caregivers of people with AIDS, age-related dementias, and advanced-stage cancers. Perspect Psychiatr Care. 2000;36:121-30.
- [Google Scholar]
- Symptom burden and quality of life in survivorship: A review of the literature. Cancer Nurs. 2015;38:E29-54.
- [Google Scholar]
- Knowledge of and barriers to pain management in caregivers of cancer patients receiving homecare. Cancer Nurs. 2007;30:31-7.
- [Google Scholar]
- The impact of serious illness on patients' families. SUPPORT investigators. Study to understand prognoses and preferences for outcomes and risks of treatment. JAMA. 1994;272:1839-44.
- [Google Scholar]
- Family caregiver burden: Results of a longitudinal study of breast cancer patients and their principal caregivers. CMAJ. 2004;170:1795-801.
- [Google Scholar]
- Psychosocial aspects of caregiving: Perceptions of cancer patients and family caregivers. Support Care Cancer. 2012;20:349-56.
- [Google Scholar]
- Quality of life and mental health in family caregivers of patients with terminal cancer. Support Care Cancer. 2011;19:1519-26.
- [Google Scholar]
- Economic burdens and quality of life of family caregivers of cancer patients. Oncology. 2005;68:107-14.
- [Google Scholar]
- The relationship of the quality of life and burden of informal caregivers of patients with cancer in Lima, Peru. J Nurs Educ Pract. 2016;6:36-42.
- [Google Scholar]
- Family caregivers' burden: A hospital based study in 2010 among cancer patients from Delhi. Indian J Cancer. 2015;52:146-51.
- [Google Scholar]
- Reliability and validity of Turkish version of the caregiver quality of life index cancer scale. Asian Pac J Cancer Prev. 2013;14:4415-9.
- [Google Scholar]
- Effects of care burdens of caregivers of cancer patients on their quality of life. Asian Pac J Cancer Prev. 2012;13:4141-5.
- [Google Scholar]




