
Translate this page into:
Hypnotic Intervention for Unexplained Dizziness in Patients with Advanced Cancer: A Preliminary Retrospective Observation Study
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Patients with advanced cancer rarely complain of unexplained dizziness after excluding identifiable causes. Some patients become anxious because they attribute the dizziness to the progression of their cancer. We hypothesize that unexplained dizziness is associated with neck muscle hypertonicity, a noncancer-related secondary effect. However, most cases are associated with neck muscle hypertonicity, a noncancer-related secondary effect.
Aims:
We evaluated the usefulness of hypnotic intervention that made patients aware of the relation between dizziness and neck muscle hypertonicity through the experience of muscle relaxation and recognition of muscle tension.
Settings and Design:
Advanced cancer patients requiring palliative care with unexplained dizziness who received the intervention to induce neck muscle relaxation were retrospectively compared with patients who did not.
Subjects and Methods:
The severity of dizziness that was evaluated using a numeric rating scale and the intervention efficacy rate were compared between the hypnotic and nonhypnotic groups as the primary endpoints, 7 days after the start of the intervention. Secondary endpoints included the effect size based on dizziness handicap inventory (DHI) scores before and after the intervention, and changes in patients’ awareness of the cause of dizziness.
Results:
The hypnotic intervention had a significantly greater efficacy rate (0.67, 95% confidence interval: 0.46–0.88) than the nonhypnotic intervention (0.26, 95% confidence interval: 0.08–0.44). DHI scores, especially on the emotional subscale, showed significant improvement after the intervention, and 71% of the patients were aware that neck muscle hypertonicity was the cause of dizziness.
Conclusions:
The rapid improvement in dizziness in the hypnotic group was considered to result from a change in patients’ awareness of self-manageable neck muscle hypertonicity as the cause of dizziness.
Keywords
Advanced cancer
awareness
dizziness
hypnosis
secondary neck muscle hypertonicity

INTRODUCTION
Patients with advanced cancer rarely complain of unexplained somatic symptoms for which no direct cause can be determined. Few studies have evaluated the cause and treatment of nonorganic somatic symptoms in patients with cancer.[1] Somatoform disorder and anxiety disorder are used as psychiatric diagnoses for unexplained somatic symptoms, and they are difficult to ameliorate.[2] No psychiatric and psychological intervention for unexplained somatic symptoms has yet been established in patients with advanced cancer.
One of the unexplained somatic symptoms that such patients suffer from is dizziness, which is often related to psychological stress. Stress is closely associated with endolymphatic water metabolism, which complicates the relation between dizziness and its systemic effects.[34] Complicated dizziness should be treated with a combination of psychological and physical interventions, yet most patients demonstrating psychosomatic symptoms are reluctant to receive psychological treatment.[5] A previous report showed that 83% of patients with advanced cancer were positive about accepting a physical interventions.[6] Secondary neck muscle hypertonicity has been observed in patients with dizziness, and its relation with shoulder stiffness and the feeling of cervical heaviness has been addressed. Neck muscle hypertonicity increases to stabilize the static posture resulting from vestibular compensation.[7] There is no report on association between dizziness and neck muscle hypertonicity in patients with cancer. We hypothesize the existence of secondary neck muscle hypertonicity as a cause of unexplained dizziness in patients with cancer. The hyperactivation of the muscle spindle deep in the neck has been considered as a possible mechanism for neck muscle hypertonicity-induced dizziness.[8] There is also a possible relation between the muscle spindle and the myofascial trigger point, which is a typical pathologic finding in myofascial pain syndrome.[9] The myofascial pain syndrome is recognized in the neck to 11.9% 1 year after curative treatment of head and neck cancer.[10] The myofascial trigger points are reported to be in 31% of advanced cancer patients, and one-third was in the neck.[11] It has been reported that emotional factors such as anger and psychological distress, and psychosocial factors such as insomnia, may constitute important myofascial trigger points risk factors.[1213]
Some patients with advanced cancer tend to consider the development of somatic symptoms as a sign of cancer progression, resulting in increased anxiety. A study that focused on patient-related barriers to opioid use reduced patients’ anxiety by addressing their misconception that pain is an indication of the progression of disease.[14] Behavioral intervention is a useful approach for changing patients’ awareness.[15] In terms of the psychosocial approach to pain management in patients with cancer, techniques aiming at behavioral change and the acquisition of coping skills are recommended.[16] These techniques include hypnotherapy, biofeedback therapy, and relaxation. To the best of our knowledge, no published studies have evaluated behavioral interventions for patients complaining of unexplained dizziness.
In this study, we used behavioral intervention to effectively change patients’ attributions of the cause of dizziness. In the intervention, patients were encouraged to experience muscular relaxation with hypnosis and to recognize the existence of neck muscle hypertonicity. We then attempted to make patients aware of the relation between dizziness and neck muscle hypertonicity, which is independent from cancer [Figure 1].
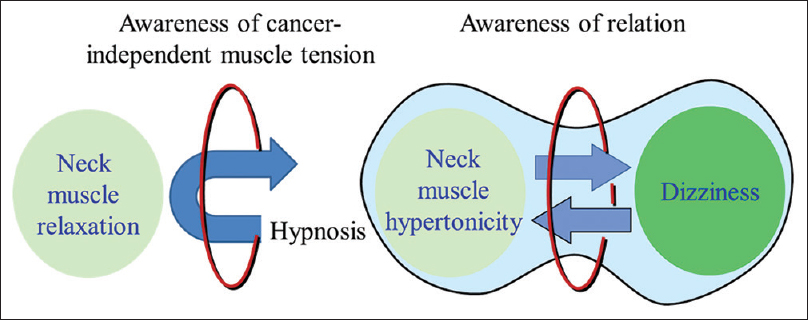
- Schematic diagram of the intervention
SUBJECTS AND METHODS
This study was performed as a preliminary retrospective observational analysis. The aim was to evaluate the usefulness of hypnosis to develop awareness in patients with advanced cancer with dizziness.
The medical records of patients who received palliative care and complained of unexplained dizziness for at least 7 days were collected. We compared two patient populations: those who were encouraged to experience muscular relaxation with hypnosis and to recognize the existence of neck muscle hypertonicity (hypnotic group) and those who were encouraged to recognize the existence of neck muscle hypertonicity with linguistic explanation (nonhypnotic group). The medical records extracted for the study included demographic factors, Eastern Cooperative Oncology Group Performance Status, and the time course and severity of dizziness in both groups. Information on patients’ awareness of the cause of dizziness, the primary tumor, concomitant treatment, days to live after initiation of the intervention, and subsequent outcome was also extracted from the records of the hypnotic group. The study subjects were hospitalized at Akaiwa Medical Association Hospital or its related medical facilities from April 2009 to March 2016. "Unexplained dizziness" was determined when the patient did not have a previous history of dizziness, and the health-care provider did not find an organic cause within 7 days after the onset of dizziness.
On the 1st day of the intervention, patients in both groups were told that "neck muscle hypertonicity is one cause" of dizziness and were taught a progressive muscle relaxation technique. Patients in the awareness intervention group received hypnosis to induce neck muscle relaxation. One of the authors, HH, performed hypnosis in the hypnotic or hypnoidal state, depending on the level of muscle relaxation and the advent of catalepsy. The hypnosis in this study was performed as a single session without the clinical application technique. During the intervention period, patients in both groups received general clinical care and psychotherapy.
The primary endpoints in this study were the difference in severity of dizziness and the intervention efficacy rate between the two groups 7 days after the start of the intervention. The severity of dizziness was evaluated using a 0–10 numeric rating scale (NRS-11). The efficacy rate was evaluated in the same manner as the severity of pain,[17] based on the percentage of patients who demonstrated a reduction of ≥33% in the severity of dizziness. The first secondary endpoint was the change in baseline dizziness handicap inventory (DHI) scores 7 days after the start of the intervention. The DHI is a self-report questionnaire that assesses the effect of dizziness on daily life activities. It consists of 25 items grouped into three subscales: physical (DHI-P, 7 items), emotional (DHI-E, 9 items), and functional (DHI-F, 9 items). Each items is scored from 0 to 4, with a maximum total score of 100. Higher scores indicate more severe dizziness.[18] Another secondary endpoint was the change in patients’ awareness of the cause of dizziness in both groups. Before and after the 7-day intervention, one of the authors, HH, asked patients "What do you think causes your dizziness?"
The change in the severity of dizziness was statistically analyzed using one-way repeated measures ANOVA for each group. The between-group difference in the change in severity of dizziness was compared using two-way repeated measures ANOVA. DHI scores before and after the intervention were compared using the paired t-test, followed by calculation of the effect size (γ). A large effect size was defined as >0.50, a medium effect size between >0.30 and ≤0.50, and a small effect size between >0.10 and ≤0.30.
Statistical analyses were performed using SigmaStat Version 3.5 statistical software (SPSS Inc., Chicago, IL, USA). P < 5% were considered statistically significant. An NRS score of 10 was applied to patients who dropped out of the study.
RESULTS
The hypnotic group included 21 patients, of whom 43% were male. Patients in the hypnotic group had a median age of 64.6 years (range: 40–81 years range) and a mean performance status of 2.6 (standard deviation [SD] = 0.7). The patients lived an average of 67.9 days (SD = 48.4) after eliminating two patients who survived until the end of the study period [Table 1]. The nonhypnotic group included 23 patients, of whom 35% were male. Patients in the nonhypnotic group had a median age of 65.3 years (range: 38–82 years) and mean performance status of 2.3 (SD = 0.9). Within 7 days after the start of the intervention, one patient from each group dropped out.

Changes in severity of dizziness and comparison of the efficacy rate between the two groups
NRS scores in hypnotic group were 7.2 (SD = 2.3) at baseline and 3.4 (SD = 3.1) and 3.3 (SD = 3.0) after 3 and 7 days, respectively. NRS scores in the nonhypnotic group were 6.7 (SD = 1.8) at baseline and 6.2 (SD = 2.6) and 7.1 (SD = 2.3) after 3 and 7 days, respectively. The efficacy rates after 7 days were 0.67 (95% confidence interval: 0.46–0.88) in the hypnotic group and 0.26 (95% confidence interval: 0.08–0.44) in the nonhypnotic group. In the hypnotic group, the change in the NRS score from baseline was significant at 3 days (P = 0.003) and 7 days (P < 0.001) after the start of the hypnosis. However, the change in NRS scores between 3 and 7 days was not significant (P = 1.000). NRS scores in the nonhypnotic group did not significantly change after 3 days (P = 0.356) or 7 days compared with the baseline (P = 0.875). A between-group comparison showed a significant difference in the change in NRS scores after the start of the intervention (P < 0.001), [Figure 2].
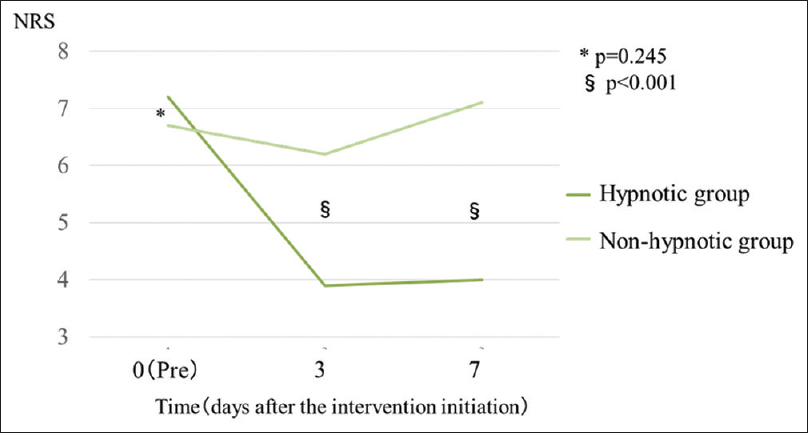
- Changes in numerical rating scale scores over time in the hypnotic and nonhypnotic groups. *, §: P value refers to the between-group comparison
Dizziness handicap inventory scores and effect sizes before and after the start of hypnosis
The overall DHI score was significantly improved by the intervention with a medium effect size [Table 2]. There were significant improvements in the DHI-P and DHI-E subscale scores, with a medium and large effect size, respectively. No significant change was observed in the DHI-F subscale.

Change in patients’ awareness of the cause of dizziness
Before the hypnotic intervention, 42% of patients had a vague sense that their dizziness might be related to the progression of cancer, 24% attributed it to the side effects of chemotherapy, 24% to an unknown cause, and 10% to meningeal dissemination due to the progression of cancer. However, after the intervention, 71% of patients believed that the potential cause of dizziness included neck muscle hypertonicity, 14% had a vague sense that it was related to the progression of cancer, 10% attributed it to an unknown cause, and 5% to hemorrhage due to the progression of cancer.
Before the nonhypnotic intervention, 52% of patients had a vague sense that their dizziness might be related to the progression of cancer, 17% attributed it to an unknown cause, 13% to meningeal dissemination due to the progression of cancer, 9% to the side effects of chemotherapy, and 9% to neck muscle hypertonicity. However, after the intervention, 35% of patients had a vague sense that their dizziness was related to the progression of cancer, 26% attributed it to an unknown cause, 17% to neck muscle hypertonicity, 13% to the side effects of chemotherapy, and 9% to meningeal dissemination due to the progression of cancer.
DISCUSSION
This is the first study to evaluate an awareness intervention in patients with advanced cancer complaining of unexplained dizziness.
The first important finding of this study was that the intervention significantly ameliorated the severity of dizziness within a short period. The majority of patients was in the terminal stage of cancer and lived an average of 67.9 days after the start of the intervention. The mean DHI score in the intervention group was 52.6, indicating severe dizziness. Patients’ awareness of the cause of dizziness was also corrected within a short period, which may have significantly ameliorated the problem.
All of the potential causes of dizziness that the patients had considered before the intervention were unmanageable factors. After the hypnotic intervention, 71% of patients attributed the cause of their dizziness to neck muscle hypertonicity, which is a self-manageable problem. Patients’ awareness of neck muscle hypertonicity as the cause of dizziness reduced their anxiety and increased their self-efficacy. Indeed, the magnitude of improvement was greater for the DHI-E than for the DHI-P and DHI-F subscales, which indicated a significant improvement in the emotional domain. In palliative care, there has been a focus on psychological interventions to improve the self-management of symptoms, for example, by reducing anxiety.[19] Symptom self-management has been reported to improve self-efficacy in patients with cancer.[2021] Self-efficacy in patients with cancer is an interactive factor between physiological status and psychological distress.[22]
A previous report showed that the expectation of reduced pain affects the prognosis of pain in cancer patients.[23] The results of this study show that patients who expected their pain to decrease had significantly lower pain intensity NRS after a week. The symptoms of pain and dizziness in advanced cancer are complex, and many factors potentially influence the outcome of the intervention. In this study, we considered that the expectation from self-management of symptoms was one of the most important factors influencing the prognosis of dizziness.
Another important finding was that the hypnotic intervention brought about rapid changes in patients’ awareness of the cause of their symptoms. Behavioral intervention is more effective for changing patients’ awareness than psychological therapy with verval explanation.[15] However, changing patients’ awareness of the cause of symptoms within a short period is not easy in the terminal stage of cancer. Progressive muscle relaxation is the most commonly used behavioral intervention in patients with cancer. However, there have been few randomized controlled studies on progressive muscle relaxation in patients with cancer,[24] and no reports on whether it can change patients’ awareness.
In this study, we used a physiological feedback mechanism in which patients experienced muscular relaxation induced by hypnosis. Hypnosis, which is a behavioral intervention, can effectively stabilize the autonomic nerve system by inducing deep muscular relaxation and an altered state of consciousness. Hypnosis has the advantage of easily enabling patients to experience physiological changes. For patients with poor self-awareness of muscle tension, the experience of physiological change is surprising and promotes self-awareness of their physiological status. The patients in our study were considered to have changed their awareness through recognition of muscle tension, which led them to understand the relation between dizziness and neck muscle hypertonicity. To the best of our knowledge, no studies have evaluated the effect of hypnosis on chronic dizziness. Although studies have evaluated the outcomes of autogenic training, including self-hypnosis for chronic dizziness and hypnosis for tension headaches, its usefulness or mechanism has not yet been established.[2526]
This study has several limitations. First, the symptoms of dizziness in advanced cancer are complex and many factors could affect the outcome of the intervention. We expected that the self-management of symptoms was one of the most important factors influencing the prognosis of dizziness. Second, this study was retrospective study. This study was not blinded because the first author was the primary palliative care physician for the study participants, and also collected and analyzed the data. Finally, an objective evaluation using an electroencephalogram was not performed. Therefore, the consistency or reliability of the depth of hypnosis was not established. Based on these limitations, this study is considered to be preliminary.
CONCLUSIONS
The rapid improvement in dizziness in the hypnotic group was considered to result from a change in patient's awareness of self-manageable neck muscle hypertonicity as the cause of dizziness.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Factors correlated with dyspnea in advanced lung cancer patients: Organic causes and what else? J Pain Symptom Manage. 2002;23:490-500.
- [Google Scholar]
- Anxious, introverted personality traits in patients with chronic subjective dizziness. J Psychosom Res. 2014;76:80-3.
- [Google Scholar]
- Antidiuretic hormone and psychosomatic aspects in Menière's disease. Acta Otolaryngol Suppl. 1997;528:109-12.
- [Google Scholar]
- The prevalence of ‘alexithymic’ characteristics in psychosomatic patients. Psychother Psychosom. 1973;22:255-62.
- [Google Scholar]
- Cancer patients’ perceptions regarding the value of the physical examination: A survey study. Cancer. 2014;120:2215-21.
- [Google Scholar]
- Objective evaluation of neck muscle tension and static balance in patients with chronic dizziness. Acta Otolaryngol. 2012;132:1168-71.
- [Google Scholar]
- Myofascial pain syndrome: Electromyographic changes associated with local twitch response. Arch Phys Med Rehabil. 1985;66:314-7.
- [Google Scholar]
- Myofascial pain syndrome after head and neck cancer treatment: Prevalence, risk factors, and influence on quality of life. Head Neck. 2015;37:1733-7.
- [Google Scholar]
- Factors associated with the efficacy of trigger point injection in advanced cancer patients. J Palliat Med. 2017;20:1085-90.
- [Google Scholar]
- Alexithymia, anger and psychological distress in patients with myofascial pain: A case-control study. Front Psychol. 2013;4:490.
- [Google Scholar]
- Myofascial trigger points, pain, disability, and sleep quality in patients with chronic nonspecific low back pain. Pain Med. 2013;14:1964-70.
- [Google Scholar]
- An oriental point of view in psychosomatic medicine. Psychother Psychosom. 1986;45:118-26.
- [Google Scholar]
- Psychosocial approach to pain management in patients with cancer. MD Anderson Manual of Psychosocial Oncology. New York: McGraw Hill; 2011. p. :165-78.
- [Google Scholar]
- Defining the clinically important difference in pain outcome measures. Pain. 2000;88:287-94.
- [Google Scholar]
- The Japanese version of the dizziness handicap inventory as an index of treatment success: Exploratory factor analysis. Acta Otolaryngol. 2011;131:817-25.
- [Google Scholar]
- Early palliative care in advanced lung cancer: A qualitative study. JAMA Intern Med. 2013;173:283-90.
- [Google Scholar]
- Perceived self-efficacy and pain control: Opioid and nonopioid mechanisms. J Pers Soc Psychol. 1987;53:563-71.
- [Google Scholar]
- The development and testing of an instrument for perceived self-efficacy for fatigue self-management. Cancer Nurs. 2011;34:167-75.
- [Google Scholar]
- Self-efficacy, depression, and physical distress in males and females with cancer. Am J Hosp Palliat Care. 2010;27:518-25.
- [Google Scholar]
- Expectation of a decrease in pain affects the prognosis of pain in cancer patients: A Prospective cohort study of response to morphine. Int J Behav Med. 2017;24:535-41.
- [Google Scholar]
- The use of relaxation for the promotion of comfort and pain relief in persons with advanced cancer. Contemp Nurse. 1994;3:6-12.
- [Google Scholar]
- Outcomes of autogenic training for patients with chronic subjective dizziness. J Psychosom Res. 2012;72:410-1.
- [Google Scholar]
- Hypnosis and autogenic training in the treatment of tension headaches: A two-phase constructive design study with follow-up. J Psychosom Res. 1992;36:219-28.
- [Google Scholar]




