
Translate this page into:
Assessment of Distress among Patients and Primary Caregivers: Findings from a Chemotherapy Outpatient Unit
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Chemotherapy is one of the treatment modalities for cancer. The side effects of treatment, at times, can affect the emotional well-being of patients and their caregivers, thereby leading to distress. This paper aims at screening and identifying levels of distress among patients undergoing chemotherapy and their caregivers.
Subjects and Methods:
A cross-sectional study design was used. Patients (n = 102) undergoing chemotherapy in the outpatient daycare unit and their caregivers (n = 101) were screened for distress using the National Comprehensive Cancer Network distress thermometer and the problem checklist. Data were analyzed using descriptive and inferential statistics.
Results:
Patients (53.4%) and their caregivers (22.2%) reported experiencing moderate-to-severe levels of distress. Patients reported significant distress in the areas of physical (P = 0.000) and emotional problems, whereas caregivers reported distress in the areas of family (P = 0.000) and emotional problems. There was no significant difference in emotional problems (P ≥ 0.05) between the patients and their caregivers. There was a positive correlation between physical and emotional problems (r = 0.760, P = 0.000). Majority of patients (85.2%) and caregivers (80.1%) showed interest to avail psycho-oncology services.
Conclusions:
Distress is prevalent among patients with cancer undergoing chemotherapy and their caregivers. Clinical implications highlight the need to identify and address caregiver distress during routine distress screening for patients using specific psychosocial interventions. Future research warrants the use of administering specific assessments to identify severe psychological issues, such as depression and anxiety for patients reporting severe levels of distress on the screening tool.
Keywords
Caregivers
chemotherapy
distress
psycho-oncology

INTRODUCTION
Distress is defined by the National Comprehensive Cancer Network (NCCN) as a “multi-factorial unpleasant emotional experience of a psychological (cognitive, behavioral, emotional), social, and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment. Distress extends along a continuum, ranging from common normal feelings of vulnerability, sadness, and fears to problems that can become disabling, such as depression, anxiety, panic, social isolation, and existential and spiritual crisis.” The NCCN in its distress management guidelines focuses on the need for screening of distress for patients diagnosed with cancer at every stage of the illness.[1]
An Indian study found that patients (23%) diagnosed with cancer (irrespective of type or stage of cancer) reported moderate-to-severe levels of anxiety and depression on the hospital anxiety and depression scale, leading to emotional distress.[2] Another study of breast cancer patients in Rome found that patients undergoing neoadjuvant chemotherapy reported higher levels of distress, leading to anxiety and depression when compared to patients planned for primary surgery.[3]
Evidence also suggests that distress is commonly experienced by caregivers, as well. A study conducted with an aim of understanding caregiver distress in early phases of cancer while patients were still receiving chemotherapy revealed that caregivers had high levels of anxiety and depression, financial burden, and lesser time for recreational activities, leading to significant distress.[45] Cal et al. studied experiences of caregivers whose spouses were diagnosed with colorectal cancer receiving chemotherapy reported issues pertaining to facing the disease (encounter with cancer, hopelessness), difficulties encountered (care burden, burnout, changes in social life), continuing to live (social support, spiritual approach, tolerance), and provision of healthcare services (need for health care staff, need for home visits).[6]
Even though there are studies that highlight the psychological impact of chemotherapy on patients and caregivers, there are sparse data available from an Indian population. Therefore, we aimed to assess levels of distress experienced by patients receiving chemotherapy and their caregivers at the outpatient daycare unit of a tertiary cancer hospital.
SUBJECTS AND METHODS
Study design
A cross-sectional design with a purposive sampling method was used.
Setting
The study was conducted at a tertiary cancer hospital located in Bengaluru, Karnataka, India. The outpatient daycare unit of the hospital is routinely involved in administering chemotherapy and other procedures (injections, hormone therapy) that do not require a patient to stay overnight. The entire chemotherapy process takes between 3 and 6 hours depending on the protocol that has been planned by the medical oncologist. While chemotherapy is being administered to the patient, the accompanying caregiver can either sit with the patient (bedside) or wait in the outpatient waiting area outside the daycare unit.
Participants
A total of 207 (105 patients and 102 caregivers) individuals were screened for distress between February and April 2018. All patients and caregivers aged above 18 years were included; pediatric patients and patients admitted for other procedures except chemotherapy were excluded.
Screening tool
We used the NCCN Distress Thermometer (DT) and problem checklist, a validated tool to assess the levels of distress and the problem categories affecting their distress. The screening tool has two parts. The first part comprises the DT, a graphical representation of thermometer marked from 0 to 10 representing the intensity of distress (0 = no distress and 10 = extreme/severe distress). The second part comprises the problem checklist, which consists of 39 items. It is divided into five different categories (practical problems, family problems, emotional problems, spiritual/religious problems, and physical problems). For the purpose of this study, the tool was translated, face validated, and back-translated to Kannada, Tamil, and Hindi (local South Indian languages) to ease in the process of comprehension.
Study procedure
Before screening the participants for distress, consent was obtained, and demographic details were collected. The NCCN-DT and problem checklist were first given to the patients to complete after which it was given to their caregivers. The tool was self-administered, and participants took approximately 3–5 min to complete the screening.
All participants who reported a score of 4 and higher, indicating moderate-to-severe distress, were encouraged to meet the psycho-oncology professional for individual sessions.
Statistical analysis
Demographic characteristics of the participants were summarized using descriptive statistics that included frequencies, mean, percentages, and standard deviation. Levels of distress and its association with problem areas of participants were analyzed using inferential statistics (Chi-square, cross-tab analysis, and Pearson product-moment correlation). The data were analyzed using SPSS, Version 17. All P ≤ 0.05 was considered statistically significant.
Ethical approval
Ethics approval for the study was obtained from the Clinical Research Business Review Team of the hospital.
RESULTS
Of the 207 participants (105 patients and 102 caregivers) who were approached, 203 (102 patients and 101 caregivers) were included for the study. Three patients were excluded as they were admitted to the daycare for procedures other than chemotherapy. One caregiver was excluded due to prior commitments.
Participant characteristics
Most of the patients (64.7%) were above the age of 50, female (63.7%), and married (93.1%). Majority (91.1%) of the patients had completed their formal education, of which 56.8% were unemployed. Breast cancer (41.2%) was the most common diagnosis. Majority of patients (72.5%) who received chemotherapy was treated with a curative intent. A significant number (85.2%) of patients reported preference to avail psycho-oncology services to manage their distress. Most of the caregivers (68.3%) were below the age of 50. Majority (95%) of the caregivers had completed a formal education, of which 72.2% were employed. Of the caregivers, majority were spouses (44.1%) and were male (51.4%) who were found to be involved in caregiving. Again, a significant number of caregivers (80.1%) reported preference for availing psycho-oncology services to manage distress [Table 1].
| Demographic characteristics | Patients (n=102), n (%) | Caregivers (n=101), n (%) |
|---|---|---|
| Age (years) | ||
| <50 | 36 (35.2) | 69 (68.3) |
| >50 | 66 (64.7) | 32 (31.6) |
| Gender | ||
| Male | 37 (36.2) | 52 (51.4) |
| Female | 65 (63.7) | 49 (48.5) |
| Marital status | ||
| Married | 95 (93.1) | 90 (89.1) |
| Unmarried | 6 (5.88) | 11 (10.8) |
| Widow | 1 (0.98) | 0 (0.0) |
| Education | ||
| Formal education* | 93 (91.1) | 96 (95.0) |
| No formal education | 9 (8.8) | 5 (4.9) |
| Employment status | ||
| Employed** | 43 (42.1) | 73 (72.2) |
| Not employed*** | 58 (56.8) | 28 (27.7) |
| Preference toward psycho-oncology services | ||
| Yes | 87 (85.2) | 81 (80.1) |
| No | 15 (14.7) | 20 (19.8) |
| Diagnosis | ||
| Breast cancers | 42 (41.2) | |
| Gastrointestinal cancersa | 18 (17.6) | |
| Hematological malignanciesb | 12 (11.8) | |
| Gynecological cancersc | 11 (10.8) | |
| Head and neck cancers | 7 (6.9) | |
| Lung cancer | 5 (4.9) | |
| Genitourinary cancersd | 4 (3.9) | |
| Sarcoma | 3 (2.9) | |
| Intent of treatment (chemotherapy) | ||
| Curative | 74 (72.5) | |
| Palliative | 28 (27.5) | |
| Caregiver relationship to patient | ||
| Spouse | 45 (44.1) | |
| Children | 37 (36.3) | |
| Sibling | 7 (6.9) | |
| Parent | 7 (6.9) | |
| Friends/extended family | 6 (5.8) |
*Formal education includes: School education, graduation, postgraduation, **Employed includes: Agricultural farmer/laborers, students, private sector employees, ***Not employed includes: Housewife, on sabbatical, retired persons. aStomach, pancreas, gall bladder, colon, rectum, cholangiocarcinoma, bLeukemia, lymphoms, myeloma, cOvary, cervix, endometrium, dProstate, urinary bladder
Distress levels and problem categories
Patients (53.4%) and caregivers (22.2%) reported moderate-to-severe distress (score of >4) on the NCCN-DT [Figure 1].
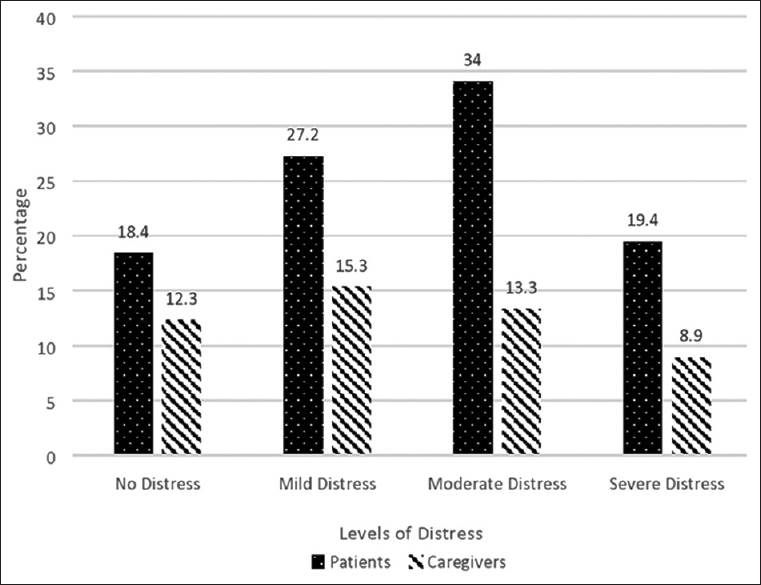
- Levels of distress experienced among patients and caregivers
Patients reported increased distress in the categories of physical problems (fatigue, pain, sleep, skin dry/itchy) and emotional problems (worry, sadness) [Figure 1].
Caregivers were found to report increased distress relating to family problems (family health issues), emotional problems (worry, sadness, fears), and physical problems (pain, sleep) [Figure 2].

- Areas of distress among patients
Association between problem categories of distress
There was a statistically significant association that was found between patients' and caregivers' overall distress levels and the problem categories of the problem checklist. Among patients, it was found that physical problems had a statistically significant association with the overall distress (P = 0.000). Fatigue (33%) was experienced by patients which had a significant impact on overall distress (Chi-square [χ2] = 29.37). Similarly, pain (30.2%) was another significant physical concern that influenced overall distress (χ2 = 13.49).
Among caregivers, family problems had a statistically significant association with the overall distress (P = 0.000). Family health issues (40.4%) were reported to influence overall distress (χ2 = 65.40) [Figure 3].

- Areas of distress among caregivers
There was no statistical difference between the patients and caregivers in the category of emotional problems (P = 0.000). Both patients and caregivers reported significant distress in the area of emotional problems. Worry was the most frequently reported problem by patients (30.7%) and caregivers (31.7%), which had an influence on their overall distress (χ2 = 0.084) [Table 2].
| Problem categories | Patients | Caregivers | ||||||
|---|---|---|---|---|---|---|---|---|
| Observed distress (%) | χ2 | Df | P | Observed distress (%) | χ2 | Df | P | |
| Family problems | ||||||||
| Dealing with partner | 4.4 | 3.56 | 1 | 0.046* | 8.9 | 3.56 | 1 | 0.046* |
| Family health issues | 12.3 | 65.40 | 1 | 0.000** | 40.4 | 65.40 | 1 | 0.000** |
| Emotional problems | ||||||||
| Worry | 30.7 | 0.084 | 1 | 0.77 | 31.7 | 0.084 | 1 | 0.77 |
| Sadness | 22.2 | 0.395 | 1 | 0.53 | 24.1 | 0.395 | 1 | 0.53 |
| Fears | 19.7 | 0.008 | 1 | 0.93 | 19.2 | 0.008 | 1 | 0.93 |
| Nervousness | 12.8 | 2.87 | 1 | 0.09 | 7.9 | 2.87 | 1 | 0.09 |
| Physical problems | ||||||||
| Fatigue | 33 | 29.377 | 1 | 0.000** | ||||
| Pain | 30.2 | 13.496 | 1 | 0.000** | 16.8 | 13.496 | 1 | 0.000** |
| Sleep | 24.1 | 6.395 | 1 | 0.015 | 15.3 | 6.395 | 1 | 0.015 |
| Skin dry/itchy | 23.2 | 17.195 | 1 | 0.000** | 1 | |||
| Eating | 21.2 | 23.549 | 1 | 0.000** | 13.8 | 23.549 | 1 | 0.000** |
*Statistically significant at P<0.05 and **P<0.01. Df: Degree of freedom
Relationship between problem categories and intent of chemotherapy (curative or palliative)
The association between the problem categories of distress and intent of chemotherapy was analyzed using Pearson product-moment correlation. Irrespective of the intent of chemotherapy received, the problem areas of distress that affected the patients and their caregivers remained the same. There was a positive correlation between physical areas of distress such as fatigue (r = 0.735, P = 0.004), pain (r = 0.682, P = 0.000), and intent of chemotherapy (curative or palliative) (r = 0.737, P = 0.000) among patients. Similarly, for caregivers, a significant correlation was observed between emotional areas of distress such as worry (r = 0.684, P = 0.000), sadness (r = 0.576, P = 0.002), and intent of chemotherapy (r = 0.760, P = 0.000) [Table 3].
| Patient-physical problems | Correlation coefficient (r) | P | Caregiver-emotional problems | Correlation coefficient (r) | P |
|---|---|---|---|---|---|
| Pain | 0.682 | 0.000** | Sadness | 0.576 | 0.002** |
| Fatigue | 0.735 | 0.004* | Worry | 0.684 | 0.000** |
| Sleep | 0.472 | 0.005* | Fears | 0.472 | 0.001** |
| Intent of chemotherapy*** | 0.737 | 0.000** | Intent of chemotherapy*** | 0.760 | 0.000** |
*Statistically significant at P<0.05 and **P<0.01, ***Curative/palliative
DISCUSSION
Our study aimed to assess distress using the NCCN-DT and problem checklist among patients receiving chemotherapy and their caregivers from an outpatient daycare unit of a tertiary cancer hospital. Both patients and caregivers were found to report moderate-to-severe levels of distress on the screening tool. However, patients reported distress in the categories of physical and emotional problems, which is consistent with studies that reported significant distress during chemotherapy in relation to patient's physical and emotional well-being.[789101112131415]
Caregivers, on the other hand, reported significant issues in the categories of family and emotional problems. Santre et al. affirmed through their study findings that more than half of caregivers (53%) reported high emotional distress on the hospital anxiety and depression scale.[16] Other studies found low self-efficacy being reported by patients and caregivers which led to higher levels of anxiety, poorer quality of life, caregiver strain, and psychological distress. There were also significant correlations between cancer patient's depression, anxiety, distress, somatization and caregiver's depression, anxiety, distress, somatization.[1718] Our findings are in line with literature, which suggests that caregivers face challenges such as processing emotions surrounding the patient's initial diagnosis or recurrence and addressing the patient's practical and emotional needs.[19]
Spouses and children were more commonly involved in caregiving in our study and reported higher levels of distress. Further, spouses (husbands of breast cancer patients) and adult children of dependent parents during the patient's treatment exhibited significant distress.[2021]
The findings of our study and earlier conducted studies emphasize that patients and their caregivers report distress on various domains on different tools. It is important to consider patients and caregivers individually for screening and then plan for appropriate interventions to reduce the reported distress. The patients and caregivers that were screened for distress in our study reported interest in availing psycho-oncology services. A study found that breast cancer patients (42%) undergoing radiotherapy had expressed interest in receiving supportive counseling to manage their distress.[22] The interest shown by patients and caregivers toward adjunct support services such as psycho-oncology shows that they are open to receiving help from mental health professionals, which is contrary to popular belief that stigma exists toward psychological support.
Our study has a number of strengths. First, the need to understand and recognize both patient and caregiver distress individually has been highlighted. Second, our participants showed interest in receiving psychological support once levels of distress were addressed. Third, having in-house psycho-oncology services can prove beneficial for providing holistic care to patients diagnosed with cancer and their caregivers. Our study has limitations of being from a single-center and the sample size may not be representative of a larger population.
Future research warrants specific assessments to identify depression and anxiety for patients and caregivers at our center. Clinical implications suggest the need to routinely screen patients and their caregivers for distress at pivotal points and provide appropriate interventions to cope effectively during chemotherapy.
CONCLUSION
Distress is prevalent among patients with cancer undergoing chemotherapy and their caregivers. Future research warrants specific assessments to identify depression and anxiety for patients and caregivers at our centre. Clinical implications suggest the need to routinely screen patients and their caregivers for distress at pivotal points and provide appropriate interventions to cope effectively during chemotherapy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
First, we are thankful to our patients and their caregivers for giving their consent for the study. We are also grateful to Dr. Sulakshana Kumar for supporting us throughout the study. We also appreciate our colleague Ms. Zeina Sravya Ahmed, who helped us in the data collection process.
REFERENCES
- Available from: https://oncolife.com.ua/doc/nccn/Distress_Management.pdf
- Prevalence of emotional distress in cancer patients. IOSR J Dent Med Sci. 2014;13:09-14.
- [Google Scholar]
- Neo-adjuvant chemotherapy and distress in breast cancer patients: The moderating role of generalized self-efficacy. J Clin Oncol. 2017;35(Suppl 15):e21570-0.
- [Google Scholar]
- Caregiving burden, stress, and health effects among family caregivers of adult cancer patients. JAMA. 2012;307:398-403.
- [Google Scholar]
- Experiences of caregivers with spouses receiving chemotherapy for colorectal cancer and their expectations from nursing services. Asia Pac J Oncol Nurs. 2017;4:173-9.
- [Google Scholar]
- 1982. Factors Contributing to Emotional Distress During Cancer Chemotherapy. Cancer Wiley Online Library; Available from: Https://onlinelibrarywileycom/doi/abs/101002/1097-0142%2819820901%2950%3A5%3C1020%3A%3AAID-CNCR2820500534%3E30CO%3B2-J
- Side effects and emotional distress during cancer chemotherapy. Cancer. 1989;63:604-12.
- [Google Scholar]
- The prevalence of psychological distress by cancer site. Psychooncology. 2001;10:19-28.
- [Google Scholar]
- Is symptom burden a predictor of anxiety and depression in patients with cancer about to commence chemotherapy? Med J Aust. 2009;190:S99-104.
- [Google Scholar]
- Quality of life, symptom experience and distress of lung cancer patients undergoing chemotherapy. Eur J Oncol Nurs. 2010;14:400-9.
- [Google Scholar]
- Psychosocial concerns in patients with advanced cancer: An observational study at regional cancer centre, India. Am J Hosp Palliat Care. 2010;27:316-9.
- [Google Scholar]
- The influence of chemotherapy-induced neurotoxicity on psychological distress and sleep disturbance in cancer patients. Curr Oncol. 2014;21:174-80.
- [Google Scholar]
- Assessment of distress among chemotherapy patients: A comparative study of gender. Paid Ribeirã Preto. 2014;24:56-65.
- [Google Scholar]
- Prevalence of emotional distress in caregiver's of cancer patients. Int J Med Res Health Sci. 2014;3:675.
- [Google Scholar]
- Self-efficacy for managing pain, symptoms, and function in patients with lung cancer and their informal caregivers: Associations with symptoms and distress. Pain. 2008;137:306-15.
- [Google Scholar]
- Care givers' depression, anxiety, distress, and somatization as predictors of identical symptoms in cancer patients. J Cancer Res Ther. 2016;12:53-7.
- [Google Scholar]
- Family caregiving challenges in advanced colorectal cancer: Patient and caregiver perspectives. Support Care Cancer. 2016;24:2017-24.
- [Google Scholar]
- Characterizing burden, caregiving benefits, and psychological distress of husbands of breast cancer patients during treatment and beyond. Cancer Nurs. 2011;34:E21-30.
- [Google Scholar]
- Psychological morbidity, burden, and the mediating effect of social support in adult children caregivers of oncological patients undergoing chemotherapy. Psychooncology. 2013;22:1587-93.
- [Google Scholar]
- Providing psychosocial support for breast cancer patients based on screening for distress within a consultation-liaison service. Psychooncology. 2004;13:893-7.
- [Google Scholar]




