
Translate this page into:
Lumbar Erector Spine Plane Block for Pain Management in Postherpetic Neuralgia in a Patient with Chronic Lymphocytic Leukemia
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Postherpetic neuralgia (PHN) refers to the chronic neuropathic pain that persists beyond the initial varicella-zoster rash. Patients with chronic lymphocytic leukemia (CLL) are susceptible to infections because of decreased immunity. Various treatment strategies including pharmacological, nonpharmacological, and interventional techniques have been described in the literature. We report the successful management of PHN with lumbar erector spinae plane block in a patient of CLL.
Keywords
Chronic lymphocytic leukemia
lumbar erector spinae plane block
neuropathic pain
nonmalignant pain
postherpetic neuralgia

INTRODUCTION
Postherpetic neuralgia (PHN) is one of the prominent causes of nonmalignant pain in chronic leukemia patients. It can occur due to the disease itself or its treatment causing reactivation of latent varicella-zoster requiring urgent pain management. Widespread PHN has a considerable effect on the quality of life.
The pain of PHN is typically described as lancinating or electric shock-like sensation along the dermatomal distribution of the rash caused by herpes zoster. Unilateral thoracic dermatomes and the ophthalmic branch of the trigeminal nerve are most commonly affected. Patchy allodynia, hyperesthesia, and hypoesthesia are also present in the affected region.
Erector spinae plane block (ESPB) is a fascial plane block which interrupts neural conduction through the spinal nerves and/or sympathetic nerve fibers. Till date, lumbar ESPB is reported to provide good analgesia in hemiarthroplasty and iliac crest bone graft donor site analgesia.[12] We describe the management of PHN with lumbar ESPB in a patient of CLL.
CASE REPORT
Our patient, a 52-year-old male (165 cm, 90 kg), was a known case of chronic lymphocytic leukemia (CLL, Rai Stage II). He had received two cycles of bendamustine and rituximab-based chemotherapy in two consecutive months. He developed herpes zoster infection in the following month and was started on oral acyclovir after consultation with a dermatologist. One week later, he visited our pain clinic and complained of severe pain on the right side of his lower back [Figure 1]. The pain was burning in nature and was associated with allodynia and restricted mobility. A diagnosis of PNH was made, and he was started on gabapentin in view of neuropathic nature of pain. The dermatomal distribution of the pain was from T11 to S1. The pain was affecting the quality of life of the patient and the pharmacological therapy was inadequate.
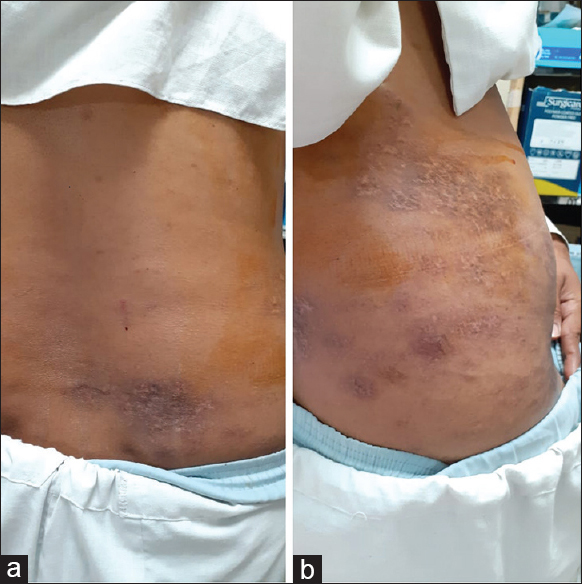
- (a and b) Herpetic lesions
We decided to perform a right-sided ESPB in prone position for acute pain relief of the patient. A high-frequency linear ultrasound probe was placed in longitudinal orientation, about 3 cm lateral to the spinous process of the third lumbar vertebra. The interfacial plane below the erector spinae muscle was identified, and 0.25% bupivacaine and triamcinolone 40 mg (total volume 30 ml) were injected [Figure 2]. Patient's NRS score was decreased from 8/10 to 3/10 30 min after the block procedure. Later on, the ESPB was performed two times for 2 weeks and provided effective analgesia for the PHN. The patient reported a decline in pain score and analgesics consumption in follow-up clinics.

- The sonographic image of lumbar erector spinae plane block. LDM: Latissmus dorsi; SPIM: Serratus posterior inferior muscle; ESM: Erector spinae muscle; LA: Local anesthetic, TP: Transverse process
DISCUSSION
Pain is a less common complaint in patients with CLL. Pain in CLL can be due to bony infiltration of lymphoblastic cells.[3] CLL patients are immuncompromised[4] and prone for the activation of latent viral infection like varicella-zoster virus. PHN is a nonmalignant cause of pain in CLL patients. The virus enters the dorsal root ganglia during the primary infection. The reactivation of virus results in the typical dermatomal distribution of pain and neural inflammation which leads to demyelination, Wallerian degeneration, and fibrosis.[5] The peripheral cutaneous nociceptors are involved in early stage, whereas the central nervous system is affected later.
Our patient received two cycles of bendamustine and rituximab-based chemotherapy which has been associated with PHN.[6] The patient had continuous debilitating neuropathic pain in the right lower back in the dermatome from T11 to S1. Pain management of PHN involves pharmacological and interventional therapies. Oral agents such as gabapentin, pregabalin, opioids, nonsteroidal anti-inflammatory drugs, and tricyclic antidepressants; intravenous such as lidocaine and ketamine; topical agents such as capsaicin cream and 5% lidocaine patch etc. have been tried for pain management. Interventions such as epidural, paravertebral block, radiofrequency ablation, and endoscopic transthoracic sympathectomy are also described in the literature with variable success rates.
Our patient had minimal relief from gabapentin and lignocaine patch. Hence, we decided to go for early intervention. Breaking the cycle of pain by interventional procedures can alleviate the symptoms and decrease analgesic consumption. ESPB has been widely used in various acute and chronic pain conditions, which is simple and can be easily performed by anatomical landmark-guided as well as ultrasound-guided techniques.[7] Thoracic erector spinae block has been used for the management of acute pain in herpes zoster and also for analgesia in PHN previously.[89] Lumbar ESPB was used in alleviating chronic low back pain in failed back surgery syndrome.[10] Lumbar ESPB with adequate local anesthetic volume and steroid was found to be effective in alleviating neuropathic pain associated with PHN in this patient. This management opens prospects on large-scale clinical studies for the applications of lumbar ESPB in chronic pain. Effective ESPB can cause a reduction in the consumption of oral analgesics.
We conclude that the lumbar ESPB for the pain management of PHN was successful and decreased the requirements of other analgesics.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Combination of lumbar erector spinae plane block and transmuscular quadratus lumborum block for surgical anaesthesia in hemiarthroplasty for femoral neck fracture. Indian J Anaesth. 2018;62:802-5.
- [Google Scholar]
- Iliac crest bone graft donor site analgesia: A new indication for erector spinae plane block. Can J Anaesth. 2019;66:338-9.
- [Google Scholar]
- IwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood. 2018;131:2745-60.
- [Google Scholar]
- Chronic lymphocytic leukemia and infection risk in the era of targeted therapies: Linking mechanisms with infections. Blood Rev. 2018;32:387-99.
- [Google Scholar]
- Post-herpetic neuralgia: A review of current management strategies. Indian J Pain. 2013;27:12-21.
- [Google Scholar]
- Infectious complications in chronic lymphocytic leukemia. Mediterr J Hematol Infect Dis. 2012;4:e2012070.
- [Google Scholar]
- Erector spinae plane block: Anatomical landmark-guided technique. Saudi J Anaesth. 2019;13:268-9.
- [Google Scholar]
- Ultrasound guided low thoracic erector spinae plane block for management of acute herpes zoster. J Clin Anesth. 2018;45:60-1.
- [Google Scholar]
- High-thoracic ultrasound-guided erector spinae plane block for acute herpes zoster pain management in emergency department. Am J Emerg Med. 2019;37:375e1-00.
- [Google Scholar]
- Erector spinae plane block for low back pain in failed back surgery syndrome: A case report. JA Clin Rep. 2018;4:60.
- [Google Scholar]




