
Translate this page into:
Oral Microbiological Evidence among Palliative Patients: An Integrated Systematic Review
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Life-limiting diseases such as cancers and its related treatments often compromise normal oral microbial flora and predispose a palliative patient to diverse oral infections. Knowledge on microbial flora in the oral cavity of patients with life-limiting diseases is essential to develop treatment options for clinical practitioners. This review aimed to systematically synthesize the published evidence on the oral microbiology of palliative patients. An integrative review was undertaken with defined search strategy from five databases with manual search through key journals and reference list. Studies included were published during the year 2000–2017 focusing on microbiological evidence associated with oral conditions among palliative patients. Candida presence was reported in the oral cavity of terminally ill patients in seven of nine articles, with Candida albicans being the predominant species. The majority of the included studies used oral swabs as a technique for isolation of the organism. This review is first to systematically synthesize the published evidence on the oral microbial flora of palliative patients, taking into account the techniques for identification of the microbiota. Larger multicenter studies may help in developing standardized clinical guidelines for the oral care of these patients.
Keywords
Cancer
Candida
microbial flora
oral care
terminally ill

INTRODUCTION
The oral cavity of humans is coated with a plethora of microorganisms.[1] Although most of these are considered as “beneficial flora” and have a useful purpose in the body, any imbalance can create a widespread havoc to general and oral health of the individual.[2] Candida species are normally present as commensals in the oral cavity with 30%–50% of a healthy individual carrying Candida albicans (C. albicans).[2] However, conditions such as chemotherapy and radiotherapy can compromise the immunity and self-renewal of epithelial cells leading to disruptions in the barriers that normally defend the host against microbial invasion, thus predisposing a patient to fungal infections.[34] The prevalence of clinical fungal infection increased by 24% among head-and-neck cancer patients pre- and postradiotherapy/chemotherapy.[5]
Existing evidence on characterizing the oral microbiology of healthy individuals[67] shows that 40% of the palliative patients lose their ability to communicate their oral health needs; therefore, they may suffer with treatable oral infections for a prolonged period of time.[8] This may contribute to the underreporting of oral infections among palliative patients, which may result in failure among health professionals to fully appreciate the problem. On the other hand, limited knowledge about oral conditions and related pathologies among palliative patients may continue to remain as a barrier for health-care practitioners to devise oral care interventions for this population.
Therefore, this systematic review aimed to synthesize the published evidence on the oral microbiology of palliative patients, with the following objectives:
-
To identify the types of microflora in the oral cavity of palliative patients
-
To identify the techniques used to investigate the microbiological presence in the oral cavity of palliative patients.
METHODS
Data sources
Search strategy was devised by the research team comprising of a dentist (JSD), a palliative nurse (MRV), a medical doctor (DR), and a health-care researcher (ZR). Five electronic databases were used: ScienceDirect, PubMed, Google Scholar, Ovid, and EBSCOhost. Manual search was also conducted through key journals and reference list. We limited our search to articles published from January 2000 to December 2017. The search terms were “oral condition” OR “oral disease” OR “dental disease” OR “mouth disease” OR “mouth condition” OR mucositis OR stomatitis OR candidiasis OR cheilitis OR xerostomia OR “periodontal disease” OR halitosis OR thrush OR “angular cheilitis” OR “denture stomatitis” OR gingivitis OR periodontitis OR “mouth ulcer” OR “aphthous ulcer” AND palliative OR terminally-ill OR “terminally ill” OR “advanced disease” OR “advanced illness” OR dying OR end-of-life OR hospice OR cancer AND treatment OR intervention OR therapy OR management OR “oral care” OR “mouth care” OR “dental management” AND “end-of-life care.”
Study selection
Inclusion criteria specified that studies must be: (1) in full text, (2) in English language – to ensure no bias in translation, (3) research articles only – to ensure the articles retrieved had gone through peer-reviewed process, (4) published between year 2000 and 2017 – to ensure up-to-date research studies of the topic, (5) focused on palliative patients, and (6) analysis on microbiological evidence of oral conditions.
Figure 1 illustrates the PRISMA flow chart of study selection process. The initial combined search identified 25,311 articles from 5 databases and 19 articles from other sources (manual searching and through references). The titles of the articles were reviewed, and duplicates were removed which resulted in 25,263 being excluded as they did not focus on oral conditions among palliative patients. The abstracts of the remaining 67 articles were read to ensure the relevance of the articles to our study. This resulted in 28 articles being excluded. Two reviewers (ZR and DR) then independently read the remaining 39 articles and coded them for inclusion or exclusion. Following the independent review, the two reviewers met to discuss preliminary findings and to reach a consensus on the studies to be included, and thirty studies were excluded. Thus, for the purpose of analysis, there were a total of nine articles.
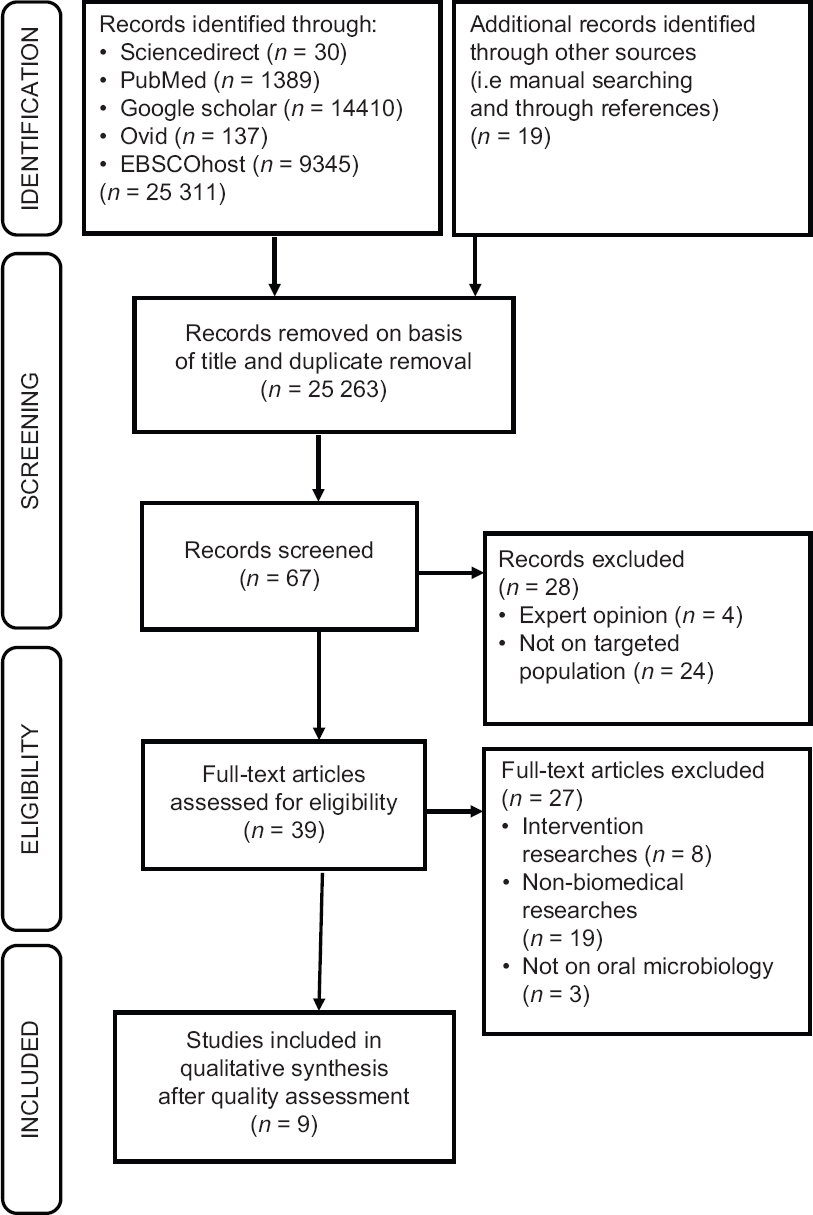
- Process of study selection
Data extraction
In the data extraction process, the study details are extracted in Table 1. This was done by two reviewers (ZR and DR). All reviewers discussed each article to reach consensus regarding the study details. The following information was extracted from each included study: author (s), year published, title, purpose, setting, origin of specimens, techniques, and microflora.
| Author (s)/year | Title | Purpose | Setting | Origin of specimens | Techniques | Microflora present |
|---|---|---|---|---|---|---|
| Davies et al./2002 | Oral yeast carriage in patients with advanced cancer | To investigate oral yeast carriage among patients with advanced cancer | United Kingdom | 120 advanced cancer patients | Isolation and identification of yeasts from oral swabs Isolation of yeasts Using Sabouraud dextrose agar and CHROMagar™ Candida Identification of yeasts Using API 20 C AUX yeast identification system, species-specific PCR and 26S rDNA gene sequencing. |
Oral yeast carriage present in 79 individuals (65.8%). Identified isolated individual species include: C. albicans, 46% C. glabrata, 18% C. dubliniensis, 5% Others <5% |
| Davies et al./2008 | Oral candidosis in community based patients with advanced cancer | To determine the epidemiology, etiology, clinical features, and microbiological aspects of oral candidosis among community-based patients | United Kingdom | 390 advanced cancer patients | Isolation and identification of yeasts from oral swabs Isolation of yeasts Using Sabouraud dextrose agar and CHROMagar™ Candida Identification of yeasts Using API 20 C AUX yeast identification system, species-specific PCR and 26S rDNA gene sequencing |
272 individuals (69.7%) had microbiological evidence of oral yeast carriage C. albicans found sole in patients (n=51) is 26 Non-C. albicans in 13 patients Mixed species in 12 |
| Sh/2011 | Oral candidiasis amongst cancer patients at Qods hospitals in Sanandaj | To determine the occurrence of oral candidiasis among cancer patients at Qods hospitals in Sanandaj. | Iran | 60 cancer patients | Isolation and identification of yeasts from oral swabs Isolation of yeasts Using Sabouraud dextrose agar and CHROMagar |
19 Candida species were isolated; C. albicans outnumbered other species and accounted for 73.7% episodes of trash |
| Jayachandran et al./2016) | Oral candidiasis among cancer patients attending a tertiary care hospital in Chennai, South India: An evaluation of clinicomycological association and antifungal susceptibility pattern | To determine the species of Candida isolated from oral cavity of patients with malignancy | India | 180 cancer patients on chemotherapy and/or radiotherapy | Two oral swabs taken over the lesions, for direct Gram staining to look for the presence of Gram-positive yeast cell and pseudohyphae, and for inoculating the specimen into Sabouraud dextrose agar | C. albicans was the predominant species isolated (94) (58%), followed by C. tropicalis (34) (20.9%) |
| Safdar et al./2001 | Prospective study of Candida species in patients at a comprehensive cancer center | To prospectively evaluated the species stratification associated with heavy colonization and systemic infection in patients at Memorial Sloan Kettering Cancer Center in New York | United States of America | 223 patients with cancer and AIDS | A germ tube test was performed for presumptive identification of C. albicans. Organisms that failed to form a germ tube were further tested by the auxanographic plate method Five to ten colonies were obtained from the primary culture and transported on Trypticase agar slants |
C. albicans was the predominant species accounting for 235/349 Candida isolates (67.3%) Among 114 non-albicans Candida spp. C. glabrata (45.6%) C. tropicalis (18.4%) C. parapsilosis (16.6%) C. krusei (9.6%) |
| Suhail Lone et al./2014 | Oral Candida colonization and infection in cancer patients and their antifungal susceptibility in a tertiary care hospital | To investigate the epidemiology of oral yeast colonization and infection among cancer patients | India | 150 cancer patients and 150 healthy controls | Oral swabs (from tongue, buccal mucosa, and labial sulcus) taken from all the participants for yeast culture by directly inoculating on HiCrome Candida differential agar | Among the cancer group, total colonization was prevalent in 50% and oral candidiasis in 30% of all cancer patients C. albicans was the most common species (74.39%) causing colonization and candidiasis with 100% susceptibility to the two azoles |
| Alt-Epping et al./2012 | Symptoms of the oral cavity and their association with local microbiological and clinical findings: A prospective survey in palliative care | To assess the subjective symptom burden and the prevalence of clinical and microbiological oral findings | Germany | 101 cancer patients | Oral swab taken from buccal mucosa, the palatal ring, and tongue for culture, followed by a mouth wash for quantitative HSV DNA testing, using PCR technique | Yeasts were found in mouth swabs of 70 patients, and HSV DNA was detected in 19 patients Presence of Candida species was 88% among the study participants |
| Davies et al./2006 | Oral candidosis in patients with advanced cancer | To determine the epidemiology, etiology, clinical features, and microbiological aspects of oral candidosis in a cohort of patients receiving specialist palliative care | United Kingdom | 120 advanced cancer patients | Isolation and identification of yeasts from oral rinses and oral swabs Isolation Using Sabouraud dextrose agar and CHROMagar Candida Identification Using API 20 C AUX yeast identification system, PCR (nested), and DNA sequencing |
79 individuals (66%) had microbiological evidence of oral yeast carriage 36 individuals (30%) had combined clinical and microbiological evidence of oral candidosis C. albicans was the predominant organism isolated from the oral swabs of patients with oral candidosis |
| Astvad et al., 2015 | OPC in palliative care patients in Denmark | To evaluate the clinical and microbiological incidence of yeast carriage/OPC | Denmark | 54 terminally ill patients | Paired samples from the buccal mucosa and the surface of the tongue were taken. The sampling included one sterile cotton swab smeared on a glass slide, fixated with methanol, followed by a sterile charcoal swab in Stuart Transport Medium | Yeast carriage rate was 83%. C. albicans accounted for half of the isolates cultured |
C. albicans: Candida albicans, C. glabrata: Candida glabrata, C. dubliniensis: Candida dubliniensis, HSV: Herpes simplex virus, OPC: Oropharyngeal candidiasis, PCR: Polymerase chain reaction
Assessment of study quality
The quality of the identified studies was assessed using Joanna Briggs Institute critical appraisal tool (a checklist for analytical cross-sectional studies) which consisted of eight questions focusing on the clarity of inclusion criteria, study subjects, setting, validity and reliability of the exposure and outcome measures, issues on confounding factors, and appropriateness of statistical analysis used.[9] Each question has a choice of “yes,” “no,” “unclear,” or “not applicable” as an answer. Then, an overall appraisal was made whether to include or exclude each study, or to seek further information, with comments. Only the articles that were agreed by all involved researchers were included in this systematic review to inform the findings.
Data analysis
Extracted data from all included studies were analyzed using the Whittemore and Knafl principles of integrative review with four stages: data reduction, data display, data comparison, and conclusion drawing and verification.[10] At data reduction stage, all nine primary sources included in the integrative review were divided into a predetermined conceptual classification aligned with the aim of this review which is microbiological presence in the oral cavity of palliative patients and its identification techniques. Each primary source was reduced to a single page (available on request from authors). This helped us to systematically compare primary sources on specific issues, variables, and sample characteristics. It also allowed us to organize data into a manageable framework.
At Stage 2 – data display, the single-page data from the nine included studies are then extracted and displayed in Table 1. This helped us to visualize the patterns and relationships between and within primary data sources.
At Stage 3 – data comparison, we used constant comparison as a method of an iterative process of examining data to identify themes that had similar patterns and relations.
Finally, at Stage 4 – conclusion and verification, we verified patterns using primary data and identified any similarities, differences, and any spurious findings. These were dealt with in order to ensure that valuable information was not lost. Five meetings were held in order to identify and reach a consensus on the final themes.
RESULTS
Characteristics of study
Overall, nine articles were found eligible and included in this review. The included study settings involved patients of advanced cancer conditions or palliative patients from five European, three Asian, and one American country. The total number of each study participants ranged from 54 to 390. The microbiological evidence of oral conditions among palliative patients of the nine eligible studies is summarized in Table 1.
Common oral microorganisms present in palliative patients
Of nine studies, seven specifically reported Candida presence in the oral cavity of palliative patients.[3111213141516] Two studies reported the presence of yeast carriage.[1718] C. albicans was the predominant species with at least 50% of the total mycological infection reported in seven of nine studies [Table 1]. Other species of Candida reported were Candida glabrata, Candida dubliniensis, Candida tropicalis, Candida parapsilosis, and Candida krusei.
Predisposing factors for oral microbial pathology among palliative patient
Two studies reported dentures, xerostomia, and oral hygiene as predisposing factors for oral microbial pathology among palliative patients.[1117] Another study reported antibiotic and corticosteroid usage as predisposing factors for Candida species infections.[15] Another prospective study considered clinical findings and laboratory findings to develop appropriate treatment strategies.[18]
Association between oral symptoms and oral microbial flora
Only three studies reported a significant association between the presence of oral symptoms and the oral microbial flora, Jayachandran et al. found a significant association between dry mouth symptom and presence of Candida species.[3] Davies reported that oral yeast carriage and denture wearing were significantly associated (P < 0.006). Similarly, there was an association between oral yeast carriage and low salivary flow rate (P < 0.009).[11] Finally, a significant association was reported between prior treatment with triazole and isolation of fluconazole-resistant C. albicans (P < 0.005), but this relationship was not observed in C. glabrata isolates (P = 0.4).[13] The other six studies reported only the mean and percentage of various Candida species.
Techniques used for identification of microbiological presence
Of the nine studies, eight studies used oral swabs to identify the microbiological presence except one,[13] where a germ tube test was used for presumptive identification of C. albicans. In five studies, Sabouraud dextrose agar and/or CHROMagar were used for isolation of microbes,[311121517] one study used Trypticase agar slants,[13] another study used HiCrome Candida differential agar,[14] and two studies did not specify the type of agar used.[1618]
Two studies adapted antifungal susceptibility test that used minimum inhibition concentration of various antifungal agents such as azoles, nystatin, and amphotericin against different isolates of Candida species.[1216]
Another two studies performed Clinical and Laboratory Standards Institute-guided microbroth dilution method to detect antifungal susceptibility.[314] Another study used the National Committee for Clinical Laboratory Standards guidelines to identify antifungal susceptibility.[13]
DISCUSSION
Our systematic review found Candida as the most common microflora in the oral cavity of palliative patients, with C. albicans being the predominant species. This finding is worrying because although C. albicans is often present as commensal in the oral cavity, their transition as an opportunistic pathogen is made possible when the host defense is compromised,[19] for example, patients undergoing chemotherapy and/or radiotherapy targeting carcinomas and sarcomas.[19] This is evident as oral candidiasis is common in head-and-neck cancer patients,[19] with 70%–75% Candida carriage in patients taking chemotherapy and/or radiotherapy.[20] A study reported that chemotherapy and/or radiotherapy causes mucositis and changes in saliva consistency. Xerostomia or thick saliva makes the oral environment conducive for fungal colonization.[21]
Oral candidiasis is also a common side effect of cancer treatments which harm the body's mucous membranes and further weaken the immune system, making it more difficult for the body to fight off the Candida infection.[1622] Studies have suggested the use of antifungal medications during cancer treatment to prevent an infection.[1622] In palliative conditions, diverse form of antifungal medications, such as mouthwashes, gels, ointments, capsules, or given as an infusion, and can help to have an effect on a limited local region (topical), on the entire body (systemic) or with a combined effect. However, no evidence is available whether these antifungal medications can help reduce other oral candidiasis symptoms such as pain or difficulty swallowing.
There are various techniques available for the isolation of Candida within the oral cavity such as the use of smear, an imprint culture, collection of whole saliva, concentrated oral rinse, and mucosal biopsy,[23] and the majority of our included studies only used oral swabs for isolation. It is a relatively simple method of detecting growth of microflora, site specific, and can obtain semi-quantitative estimation of Candida, and this technique is difficult to standardize.[23] Since Candida is the resident microflora within the oral cavity, a more reliable and appropriate isolation methods are required to ascertain its presence along with their quantity.
CONCLUSION
To our knowledge, this study is the first systematic review taking into account the techniques to identify the oral microflora among palliative patients. It is hoped that the information generated from this review will lead to a better understanding of oral conditions among palliative patients in order to direct the treatment options and enhance the quality of care for these terminally ill patients. Future studies with multicenter approach may help to develop standardized clinical guidelines for oral care of palliative patients.
Financial support and sponsorship
This study was financially supported by Universiti Brunei Darussalam, Grant information: UBD/OAVCRI/CRGWG (014)/171001.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We would like to thank Universiti Brunei Darussalam for the award of a grant that makes this project possible.
makes this project possible.
REFERENCES
- Defining the normal bacterial flora of the oral cavity. J Clin Microbiol. 2005;43:5721-32.
- [Google Scholar]
- Oral candidiasis among cancer patients attending a tertiary care hospital in chennai, South India: An evaluation of clinicomycological association and antifungal susceptibility pattern. Can J Infect Dis Med Microbiol. 2016;2016:8758461.
- [Google Scholar]
- How chemotherapy increases the risk of systemic candidiasis in cancer patients: Current paradigm and future directions. Pathogens 2016:5. pii: E6
- [Google Scholar]
- A systematic review of oral fungal infections in patients receiving cancer therapy. Support Care Cancer. 2010;18:985-92.
- [Google Scholar]
- Oral flora in independent over 80-year-olds with more than 20 teeth. Bull Tokyo Dent Coll. 2006;47:1-4.
- [Google Scholar]
- Dental treatment intensity in frail older adults in the last year of life. J Am Dent Assoc. 2013;144:1234-42.
- [Google Scholar]
- 2017. Checklist for Analytical Cross Sectional Studies Critical Appraisal Checklist for Analytical Cross Sectional Studies. Joanna Briggs Institute; Available from: http://joannabriggsorg/research/critical-appraisal-toolshtmlwwwjoannabriggsorg
- Oral yeast carriage in patients with advanced cancer. Oral Microbiol Immunol. 2002;17:79-84.
- [Google Scholar]
- Oral candidiasis amongst cancer patients at Qods hospitals in Sanandaj. 2011. Afr J Cln Exper Microbiol. 12:129-32. Available from: https://wwwajolinfo/indexphp/ajcem/article/viewFile/66913/54910
- [Google Scholar]
- Prospective study of Candida species in patients at a comprehensive cancer center. Antimicrob Agents Chemother. 2001;45:2129-33.
- [Google Scholar]
- Oral Candida colonization and infection in cancer patients and their antifungal susceptibility in a tertiary care hospital. 2014. Int J Adv Res. 2:541-50. Available from: http://wwwjournalijarcom
- [Google Scholar]
- Oropharyngeal candidiasis in palliative care patients in Denmark. J Palliat Med. 2015;18:940-4.
- [Google Scholar]
- Oral candidosis in community-based patients with advanced cancer. J Pain Symptom Manage. 2008;35:508-14.
- [Google Scholar]
- Symptoms of the oral cavity and their association with local microbiological and clinical findings – A prospective survey in palliative care. Support Care Cancer. 2012;20:531-7.
- [Google Scholar]
- The oral carriage of Candida in oral cancer patients of indian origin undergoing radiotherapy and/or chemotherapy. J Clin Diagn Res. 2016;10:ZC17-20.
- [Google Scholar]
- The oral carriage of yeasts and coliforms in patients on cytotoxic therapy. J Oral Pathol. 1984;13:390-3.
- [Google Scholar]
- Occurrence of oral Candida in irradiated head and neck cancer patients. J Oral Med. 1984;39:194-6.
- [Google Scholar]
- 2016. Oral Thrush: Prevention During Cancer Treatment. Institute for Quality and Efficiency in Health Care; https://www.ncbi.nlm.nih.gov/books/NBK367590/
- Isolation and identification of Candida from the oral cavity. ISRN Dent. 2011;2011:487921.
- [Google Scholar]




