
Translate this page into:
Comparative Impact of Nonpharmacological Interventions on Pain of Knee Osteoarthritis Patients Reporting at a Tertiary Care Institution: A Randomized Controlled Trial
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Nonpharmacological interventions (NPIs) have been advocated for knee osteoarthritis (KOA). There are many gaps in the evidence to their efficacy in India.
Aims:
The study aims to compare the impact of two packages of NPIs on various outcome variables of KOA patients.
Settings and Design:
This was a randomized controlled trial in a tertiary care hospital.
Subjects and Methods:
A study population (n = 123) of KOA patients aged 40–65 years. Stratified block randomization was done for mild or moderate KOA into two groups. Group “A” patients received a package of NPIs including a set of supervised exercise sessions, kinesthesia, balance, and agility (KBA), meditation, weight reduction advice, and weekly telephonic reminders. Group “B” patients received the same package except for KBA & meditation. Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analog scale (VAS) and performance-based measures were measured.
Analysis:
t-test and repeat measures ANOVA were undertaken.
Results:
A significant intragroup reduction in WOMAC score was seen from baseline in Group A (P = 0.00, mean difference: −9.7) as well as in Group B (P = 0.00, −12.9). There was also significant reduction inVAS scores at the end of intervention in Group A and Group B as compared from baseline (−3.62, −3.8, P = 0.00). No intergroup difference was observed in either of the scores. VAS score reduction to 0 at different stages of intervention was noticed in 46% (n = 57) cases. There was a significant intergroup difference for 50-Foot Walk Test (P = 0.055, F = 3.28) at 12 months.
Conclusion:
Both packages of NPIs were effective in providing relief in symptoms. No specific benefit of KBA or meditation was seen except for 50FWT.
Keywords
Agility
balance
kinesthesia
knee osteoarthritis
nonpharmacological intervention

INTRODUCTION
Knee osteoarthritis (KOA) is one of the common causes of disability after the fourth decade of life.[1] Pain is the most common symptom of KOA.[2] Most nonsurgical interventions for early-to-moderate KOA include the use of nonpharmacological interventions (NPIs). Many countries have elaborate KOA management protocols.[34567] Body balance system is said to be altered in KOA patients.[8] In India, there are many gaps in evidence about the efficacy of NPIs and kinesthesia, balance, and agility (KBA) for KOA patients.[9]
Hence, the present study was conducted to create an evidence for the utility of such regimens through comparison of the impact of two packages of NPIs including a set of physiotherapy exercises, KBA training, meditation, weight reduction advice, and weekly telephonic compliance monitoring. The second group had all these elements except KBA training and meditation. It was hypothesized that the two packages of NPIs would have a differential impact on the degree of relief from pain in the two groups of KOA patients.
SUBJECTS AND METHODS
Registration protocol
Clearance for conducting the trial was obtained from the Ethics Committee of Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh. The trial was registered with the ICMR trial registry (CTRI/2014/01/004270). Written informed consent was sought from the patients. Data were kept confidential.
Junior/senior resident doctors/consultants of the Orthopedics and Physical Rehabilitation Medicine (PRM) Departments of PGIMER were requested to send Grade 1, 2, and 3 KOA patients as per Kellgren–Lawrence scale[10] to intervention room after initial workup. As a routine, in PGIMER, Chandigarh, KOA patients first report to Orthopedics Outpatient Department (OPD). After clinical workup, they are referred to the PRM Department, where they are advised various physiotherapy modalities, exercises, etc., The current study is a two parallel-group randomized controlled trial (RCT). The study population comprised patients suffering from grade mild and moderate KOA who attended the Orthopedics OPD of PGIMER during 2013–2014.
The study included patients who agreed, were willing to alter their lifestyle (weight management, exercise therapy, and reduction in sedentary time), and able to comply with the planned schedule for follow-up. The study was conducted among participants who were aged 40–65 years of either gender. Forty years as the lower cutoff was selected due to the early prevalence of KOA among Indians.[11]
The study excluded patients who were due for surgery owing to deformity or intra-articular pathology, had undergone hip or one side knee replacement, had significant deformity or comorbidities needing surgery (e.g., meniscus tears), had myocardial infarction in the previous 6 months, had any other known organic disease that contraindicated safe participation in the study (e.g., cancer); had non-OA inflammatory arthropathy or any arthritic disorder (e.g., rheumatoid arthritis), used oral corticosteroids regularly, had intra-articular joint injection within 4 weeks of the study, and had excessive obesity (body mass index [BMI] >40) or any comorbidity not allowing proper exercise protocol.
Patients above 65 years were excluded as replacement surgery is mostly recommended by orthopedic surgeons after this age.[9] The present study did not include any patient over 65 years of age even if declined surgery.
Only those illiterate participants were included who had a literate caregiver at home who could read the brochure and explain its contents (mainly pictorial) to a person who cannot read.
Randomization
All eligible patients were stratified in mild or moderate KOA, as per radiological criteria, confirmed by referring consultant. Patients who met the inclusion criteria in both the strata were randomized into two groups (A and B) using the block randomization method to ensure balanced assignment (block size 4).[12] The researcher herself assigned participants to intervention groups.
Random number table was used for randomization done by a faculty member of the School of Public Health, not involved in the study.
Blinding
It was not attempted. Since in this study, the researcher administered outcome measures by herself, she was not blind to the treatments or the evaluations.[13]
Details of intervention package
Patients in the two groups received the same intervention except for KBA and meditation, which were delivered to participants in Group A only. Weekly telephonic reminders were given to patients in Group “A” and monthly in Group “B.” Reminders were given to patients who did not turn up on scheduled visits.
Development of intervention package
Patient information brochure were developed in Hindi and in English. These were circulated among consultants for consensus validity. These were then pretested in 10 KOA patients. Further need-based corrections were done as per the feedback received. A video was developed on the set of exercises used in the study. Laptop-based training was given to patients using this video. Feedback from the clinicians and physiotherapists was also obtained about this video before finalizing it for use in the study.
Contents of patient information brochure for both groups
These included a set of exercises (standing quadriceps stretch, supine hamstring stretch, short arc lift, isometric quadriceps exercise, isometric quadriceps with medial rotation of the hip, quadriceps isometrics in sitting position, hamstring isometric, and hip abduction). These were taught to the patients by the researcher under the supervision of a physiotherapist (duration ~10 min). Thereafter, return demonstration was taken from the patients, i.e., they were asked to repeat the exercises taught to them, so that corrections, if any, could be advised. Stepwise directions and repetitions are explained in the patient information brochure. These were given to patients of both the groups.
Patient information brochure for Group “A” only
These included kinesthesia, agility exercises (wedding march, backward wedding march, high knee march, sidestepping, semi-tandem walk, tandem walk, crossover walk, modified grapevine, toe walking, and heel walking), and balance training (modified Romberg exercise, stand on one foot for 30 s with eye open, and wide/narrow circle exercises).
The researcher was trained in KBA exercises by a senior physiotherapist employed at PRM Department of PGIMER. Sessions for KBA were then conducted by her in a separate room for the Group “A” cases (n = 63) only. It was a specific supervised period of ~20 min.
Customization of the set of exercises for each patient of both the groups was done in consultation with orthopedic surgeons and physiotherapists, i.e., in case, there was discomfort in doing any exercise that was not advised for the concerned patient. Out of the total scheduled 26 visits over a period of 12 months for Group “A” patients, 25 supervised sessions were held in the intervention room. Return demonstration was taken on every follow-up visit, and corrections were advised to patients. They were also advised to perform both sets of exercises at home. They were asked to maintain a logbook also to record the same.
An introductory session (duration 10 min) was held by the researcher on the first visit of each KOA patient for both the groups. It was focused on the general information about the disease (symptoms and risk factors), description of various components of the intervention package, general precautions (do's and don'ts), clarifications on myths, and misconceptions. Videos on both sets of exercises were also shown to patients in this session. It was done only at the beginning of the treatment to explain to the patient how best to practice.
Dietary counseling
Participants in both the groups with BMI ≥25 at baseline were advised on weight reduction.
NPI package to be administered was finalized in consultation with the doctor concerned as well as with the patients and their caregivers. Participants in both groups were encouraged to comply with the instructions pertaining to various components of the intervention package.
Outcome variables
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analog scale (VAS), and performance-based tools were used for the assessment. WOMAC, a self-administered measure, consisting of 24 questions was used to assess the dimensions of pain, stiffness, and function. Patients were asked to rate the categories according to the scale of difficulty (0 = none, 1 = slight, 2 = moderate, 3 = very, and 4 = extremely). The WOMAC is a valid and reliable outcome measure for KOA in Asian KOA patients.[1415] VAS used for assessment was a standard 10-cm horizontal scale. The KOA patients indicated the severity of pain by marking between terminal points, i.e., from 0 (no pain) to 10 (worst pain). Performance tests, namely 50-Foot Walk Test (50FWT), 30-s Chair-Stand Test (30SCST), and Timed Up and Go (TUG) test were used.[1617]
Patients were followed for a period of 12 months. Total 26 visits were scheduled for each patient. Visit schedule for each patient was scheduled as baseline visit (day 1), 3rd day, 7th day, 14th day, and 21st day from baseline visit; once a week for next 2 months (visits 6–13); once in fortnight for next 4 months (visits 14–21); once a month for next 4 months (visits 22–25); and endline visit (visit 26).
On every visit, return demonstration of exercises was taken from patients. Assessment of the outcome variables was performed at 1 week, 3 months, 6 months, and 12 months. For performance-based tests, assessment was performed at 3 months, 6 months, and 12 months. Patients who did not report physically in the OPD for outcome assessment were considered as lost to follow-up. As performance-based tests could not be performed on these patients at 3, 6, and 12 months, their data were not included in the analysis, even if they attended rest of the 23 visits. However for patients who reported complete relief from pain, assessment of VAS scores was done and documented.
The study did not interfere with the pharmacological treatment or any supportive therapy prescribed for KOA patients by the concerned doctors. However, such details were duly recorded during the study.
Sample size
Eligible KOA patients were divided into two groups for the RCT. The sample size was calculated based on the objective, i.e., to assess the effectiveness of a package of NPIs with meditation and KBA in obtaining relief from the pain of KOA.
A sample size of 39 patients in each group had been decided at alpha = 0.05 and power 80%. Sample size formula: N = C × (p1q1 + p2q2)/(p1 − p2)2[18]
Where, C = 7.8 (for the power of 80% and alpha = 0.05), p1 =0.3, p2 =0.6, q = 1 − p.
N = sample size in one arm = 39.
It has often been observed that chronic disease patients often leave the treatment in between, particularly if they start feeling better.[1920]
To account for such lost to follow-up, extra cases (50% of 39) of sample size in one arm were taken. Thus, there were 60 patients in each group.
Statistical analysis
Frequency, percentage, mean, and standard deviation were used for analysis. Furthermore, repeat measures ANOVA was applied for both intragroup and intergroup differences, i.e., within- and between-group differences. For WOMAC, a t-test was also used for analysis within and between the groups. Comparison between the test and control groups (intergroup) at baseline and various follow-ups was accomplished using Student's unpaired t-test. The level of significance for the comparisons was set at P < 0.05. Statistical Package for the Social Sciences (SPSS) ver 18 was used for analysis. Intention to treat principle was followed for analysis.
RESULTS
Overall, 143 potentially eligible patients were referred from the orthopedics OPD, of which 20 patients were excluded and 123 patients were allocated to two groups after block randomization, 63 patients to Group A and 60 patients to Group B [Figure 1]. There were 87 (71%) females and 36 (29%) males enrolled in the study. Overall, 31 (49%) and 20 (33%) patients completed the study in Groups A and B, respectively.
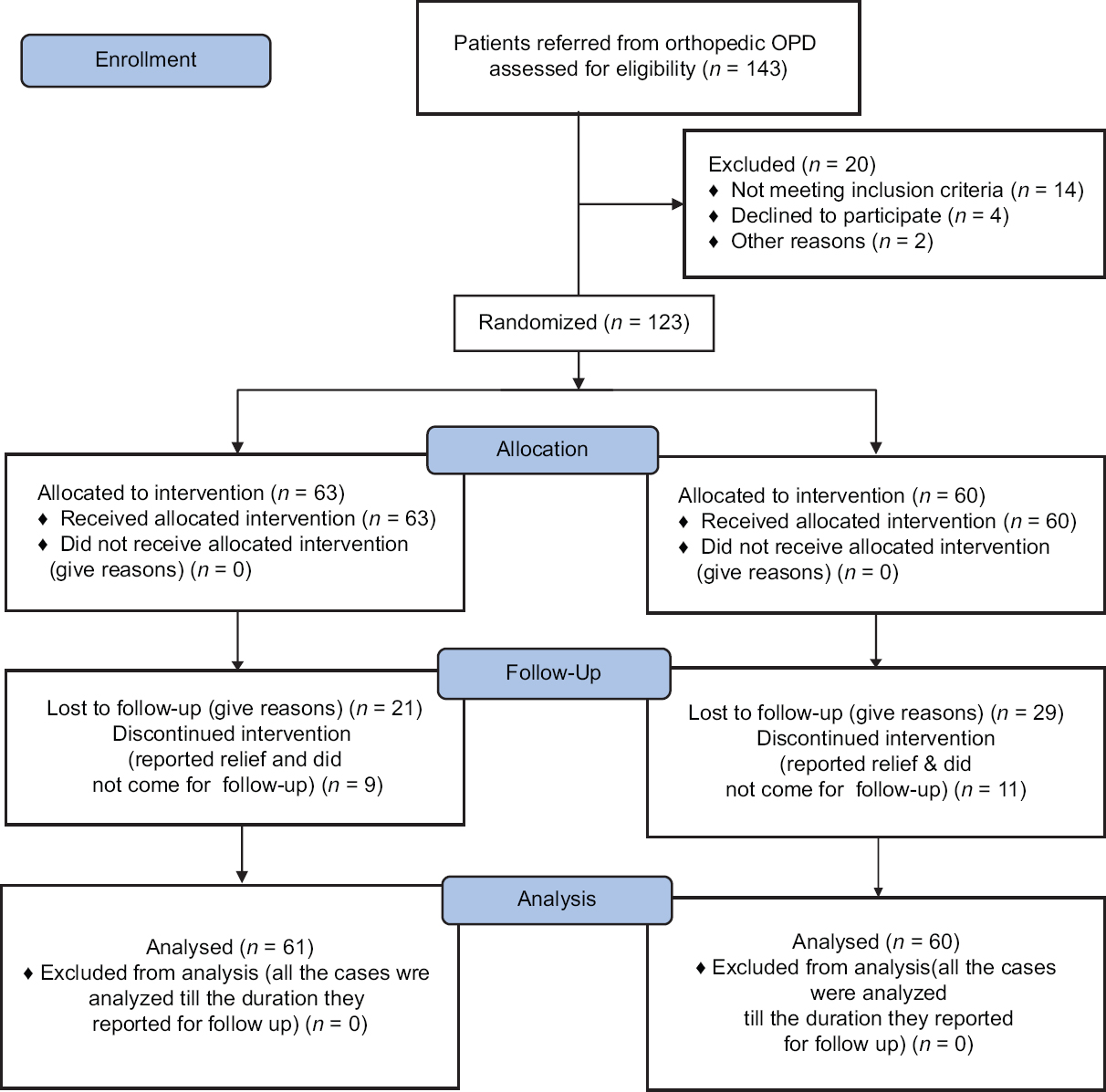
- Study design and trial attrition
There were dropouts in the first follow-up/visit (15 in Group A and 22 in Group B). Patients withdraw from a study for a reason unrelated to KOA or intervention (for example, most of them did not turn up because it was 1 day after their baseline/ first visit). They preferred to contact researcher over phone/WhatsApp, E-mail or Skype [Figure 2]. Hence, there were no systematic differences existed between dropouts and completers.
- Knee osteoarthritis patient sent exercise routine over phone/WhatsApp to researcher
However, many of these dropouts (n = 29) remained in the contact of the investigator. Five patients did not contact the investigator and discontinued the intervention package. Three reported that they have switched to complementary and alternative medicine, one reported that she took platelet-rich plasma injections, and one cited pain for discontinuation of the package. Three patients could not be contacted, as phone numbers provided by them were incorrect or phone of a distant relative was provided. These 29 patients were provided intervention package as per their groups assigned and telephonic reminders were given to them. They visited the intervention room at their will and convenience and not as per the visit schedule, but they maintained their diaries as directed by the investigator. They also reported relief in VAS and WOMAC scores as questionnaires were given to them. As per methodology, data of only those patients were included in analysis who showed up for testing of outcome variables at 1 week, 3 months, 6 months, and 12 months. Hence, data of these patients were not included in the final analysis. However, their data will be analyzed separately and published in the separate paper.
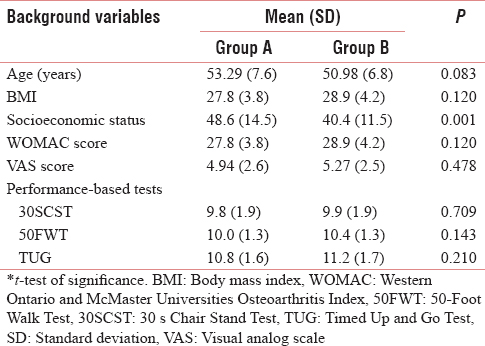
At baseline, there was no significant difference between the two groups with respect to age, height, weight, BMI, overall WOMAC score, VAS, or performance-based tests [Table 1]. WOMAC domain of pain score and socioeconomic status was significantly different in the two groups. It was assumed that protection against chance bias was taken care of by stratified randomization.[12]
At 3-month, 6-month, and 12-month follow-up visits, there were statistically significant differences “between the groups” in the 50-Foot Walk Test. No statistically significant difference was observed between the groups regarding WOMAC and VAS at the end of intervention [Table 2].
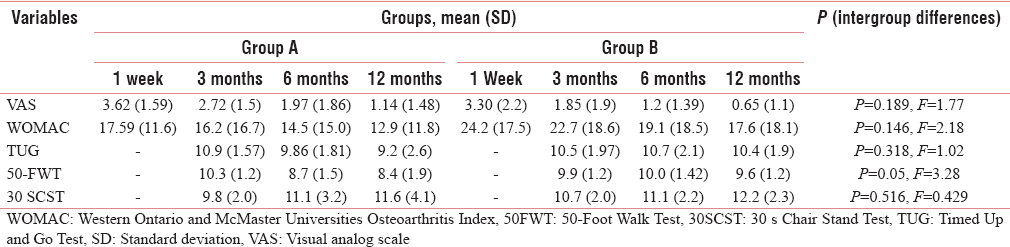
It was observed that there was the significant intragroup difference in VAS scores in Group A and Group B at the end of intervention as compared from baseline, 1 week, and 3 months (P = 0.00). In Group A, there was a significant difference at the end of intervention from baseline (P = 0.00). However, in Group B, there was a significant difference at the end of intervention from baseline, 1 week, and 3 months (P = 0.035). However, no difference was there at 6 months in comparison to 12 months [Table 3]. There was the difference in WOMAC scores within Group B at 3 months in comparison to 12 months of intervention (P = 0.001).
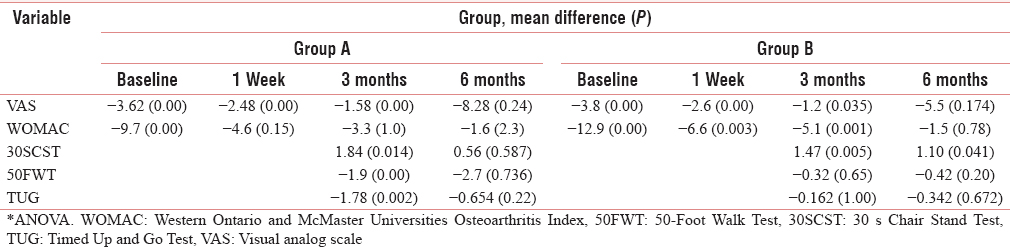
It was also observed that within Group A, there was a significant difference at 3 months in 30SCST, 50FWT, and TUG from and TUG from 12-month intervention (P = 0.014, P = 0.0, and P = 0.002). However, in Group B, there was a significant improvement in 30SCST at 12 months as compared to that at 3 months and 6 months (P = 0.005) [Table 3].
There was no statistical difference between groups' BMI at 12 months of intervention (P = 0.59). However, there was a significant improvement in the VAS scores within both the groups. Except for one case, all patients who reduced weight showed improvement in VAS, even in that weight reduction was <2 kg. A similar pattern was also observed for WOMAC where only 3 cases reported worsening (despite reduction by <2 kg).
There was a reduction in the VAS scores individually in both the groups. Overall, 57 cases (46%) reported VAS score reduction to 0 (n = 123) at different stages of intervention [Figure 3]. Some patients reported that they stopped taking analgesics (17.8%) and few reported a reduction in the frequency of analgesic intake (13.8%) after they started participating in the study.
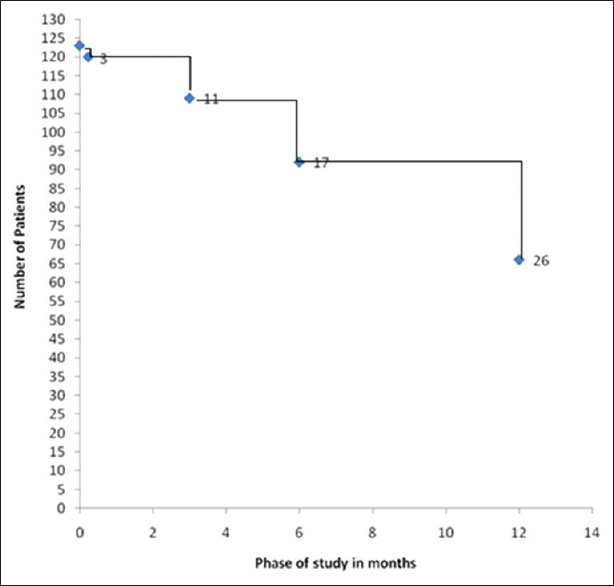
- Time taken to complete relief as per visual analog scale score (=0)
Subjective feedback from the patients also revealed appreciable benefits of the intervention. “(I have 70% relief. I have also stopped taking painkillers. So I am now really thankful to PGIMER authorities for initiating such a service. I was advised Knee Replacement by a private hospital. But now I will not go for it).”
DISCUSSION
Overall, both the NPI packages were effective in providing relief in symptoms in KOA patients. Majority (75 out of 123) patients enrolled in this study had moderate-to-severe pain initially. At the end of 12 months of intervention, only 2 patients remained in these categories; 57 patients (46%) reported complete relief in symptoms. Rest reported only mild pain at the end of the intervention phase. This relief in symptoms reported by all patients was validated through VAS and WOMAC scores. Similar favorable results of exercise and allied therapies in KOA have been reported.[21]
In follow-up visits, it was observed that 40% of patients did not do exercises correctly. Hence, return demonstration was taken on every visit. Rectification was done as and when required. In this study, the emphasis was laid upon the adequate interaction between doctors and patients. For this, an introduction session was conducted as per the convenience of patients and their family members. It helped in rapport building with them. The theme was a behavioral modification to reduce the risk of progression of KOA. Patients were informed about disease processes, medications, and their actions and reactions. The current study also emphasized on enunciating family support to the patient. Furthermore, comprehensive awareness and knowledge pertaining to the disease were provided to the patients. The investigator focused upon individualized goal setting for exercises and pain management strategies for each patient separately.
Children and spouses of the patients were also involved in the training sessions. The findings obtained in the present study suggested that the involvement of family members had a good impact on self-efficacy and motivation. The participation by family members was effective in improving compliance. This resulted in a reduction of pain and improving the health status of patients. Keefe et al. reported that an intervention using spouse-assisted coping skills training and exercise training can improve physical fitness, pain coping, and self-efficacy in KOA patients.[22]
Weight reduction is hence an important component of any intervention strategy. Even minor reductions of 3–4 kg may work wonders in relieving the symptoms. In this study also, it was seen that relief in symptoms was more when weight reduction was there. In both groups at 6 months, patients who reduced weight by 3 kg or more reported a decrease in VAS score.
The current study showed that NPIs (counseling on exercises, weight reduction, and telephonic reminders) resulted in significant improvement in WOMAC and VAS scores in both the groups (A and B). Many studies have reported the efficacy of exercises for KOA and concluded the highest level of evidence that therapeutic exercise provides benefit in pain reduction and function improvement.[23] Some studies have also reported positive effects on pain and disability in KOA with telephone contact.[24] A study concluded that after 8 weeks, a statistically significant improvement was observed in the WOMAC score of pain in the group undergoing exercise as compared with that of the control group.[25] Our the study also reported a significant reduction in pain in both groups at end of the intervention.
However, our study failed to demonstrate the statistically significant difference between the groups regarding WOMAC and VAS scores after 12 months of intervention. The possible reason could be that both groups had an almost same package of NPIs except KBA, meditation, and difference in frequency of telephonic reminders. No third control group with no active intervention was kept as it was not felt ethical to have a group that does not receive the benefit of the highest level of evidence, i.e., exercises in an intervention study of this kind.
Clark et al. study on the anterior knee pain showed that at 3 months, the WOMAC and visual analog scores improved significantly in all patients (P < 0.0001) but failed to show significant differences in score or changes in score between the four groups.[26] Our study also showed that at 3 months, there was a statistically reduction in knee pain in both the groups.
A significant difference between the groups with respect to performance-based tests (50FWT) was seen. This difference could be possible because of KBA training in Group A and weekly telephonic reminders for improving compliance.
Similar findings were indicated in the study by Rogers et al. which showed that KBA and resistance training or a combination of the two administered as home exercise programs appear to be effective in reducing symptoms and in improving the QOL among persons with KOA.[27] Few studies have been conducted in India on the effects of KBA and physiotherapy on KOA. These studies have concluded that proprioceptive training should be included along with conventional physiotherapy in KOA. However, these studies are methodologically weak. These lacked a standard control group. Sample sizes were very small.[2829]
At the end of 12 months of intervention in the present study, 57 patients (46%) of the total (n = 123) reported complete relief in pain. This could be due to explaining the conservative treatment to KOA patients through video/brochures. However, patients forgot exercises in spite of the demonstration of the same. In such situations, video/brochures were handy for guiding the patients in the correct way of doing exercises.
Another reason for a good result in our study could be organizing of supervised exercise sessions in the study. This proved to be a successful strategy. McCarthy et al. also proved that supplementation of a home-based exercise program with a class-based supervised exercise program led to clinically significant superior improvement.[30]
CONCLUSION
Patients with KOA in both groups reported statistically significant improved in knee pain and dysfunction as indicated by a within-group reduction in WOMAC and VAS scores.
No significant difference was observed in WOMAC and VAS scores between the groups after 12 months of intervention. A significant difference between the groups with respect to performance-based tests (50FWT and TUG) was seen.
Limitation
Overall, 31 (49%) and 20 (33%) patients completed the study in Group A and B, respectively. There were many dropouts in follow-up as many were reluctant to physically present in all 26 visits. Patients did not physically attend all sessions in the intervention room and preferred to contact researcher through Skype, E-mail, and WhatsApp. This should be kept in mind while interpreting the study results.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The epidemiology and impact of pain in osteoarthritis. Osteoarthritis Cartilage. 2013;21:1145-53.
- [Google Scholar]
- Determinants of pain in patients with symptomatic knee osteoarthritis. Caspian J Intern Med. 2016;7:153-61.
- [Google Scholar]
- Guideline Development Group. Care and management of osteoarthritis in adults: Summary of NICE guidance. BMJ. 2008;336:502-3.
- [Google Scholar]
- EULAR recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a task force of the standing committee for International Clinical Studies Including Therapeutic Trials (ESCISIT) Ann Rheum Dis. 2003;62:1145-55.
- [Google Scholar]
- OARSI recommendations for the management of hip and knee osteoarthritis, part I: Critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthritis Cartilage. 2007;15:981-1000.
- [Google Scholar]
- OARSI recommendations for the management of hip and knee osteoarthritis, part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008;16:137-62.
- [Google Scholar]
- American college of rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012;64:465-74.
- [Google Scholar]
- Balance impairments in individuals with symptomatic knee osteoarthritis: A comparison with matched controls using clinical tests. Rheumatology (Oxford). 2002;41:1388-94.
- [Google Scholar]
- Non-surgical Interventions and Exercises – A Guidebook for Patients. Chandigarh: New Era International Publishers; 2015.
- Severe radiographic knee osteoarthritis – Does Kellgren and Lawrence grade 4 represent end stage disease.– The MOST study? Osteoarthritis Cartilage. 2015;23:1499-505.
- [Google Scholar]
- Epidemiology of knee osteoarthritis in India and related factors. Indian J Orthop. 2016;50:518-22.
- [Google Scholar]
- Practical Statistics for Medical Research. London: Chapman and Hall/CRC; 1990.
- Getting off the “gold standard”: Randomized controlled trials and education research. J Grad Med Educ. 2011;3:285-9.
- [Google Scholar]
- Validation of the Western Ontario and Mcmaster university osteoarthritis index in Asians with osteoarthritis in Singapore. Osteoarthritis Cartilage. 2001;9:440-6.
- [Google Scholar]
- Translation and validation of the reduced Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) in Hindi speaking Indian patient with osteoarthritis of knee. Indian J Physiother Occup Ther Int J. 2010;4:37-41.
- [Google Scholar]
- Measurement properties of performance-based measures to assess physical function in hip and knee osteoarthritis: A systematic review. Osteoarthritis Cartilage. 2012;20:1548-62.
- [Google Scholar]
- OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthritis Cartilage. 2013;21:1042-52.
- [Google Scholar]
- Reasons for default from treatment of chronic illnesses in a primary healthcare program in rural Tamil Nadu. Indian J Public Health. 2013;57:173-6.
- [Google Scholar]
- Factors associated with default from treatment among tuberculosis patients in Nairobi province, Kenya: A case control study. BMC Public Health. 2011;11:696.
- [Google Scholar]
- Effectiveness of exercise therapy and its variation in lower limb Osteoarthritis: A literature review. J Postgrad Med Edu Res. 2014;48:190-6.
- [Google Scholar]
- Effects of spouse-assisted coping skills training and exercise training in patients with osteoarthritic knee pain: A randomized controlled study. Pain. 2004;110:539-49.
- [Google Scholar]
- The effect of exercise therapy on knee osteoarthritis: A randomized clinical trial. Med J Islam Repub Iran. 2015;29:186.
- [Google Scholar]
- Reduction of joint pain in patients with knee osteoarthritis who have received monthly telephone calls from lay personnel and whose medical treatment regimens have remained stable. Arthritis Rheum. 1992;35:511-5.
- [Google Scholar]
- Impact of exercise on the functional capacity and pain of patients with knee osteoarthritis: A randomized clinical trial. Rev Bras Reumatol. 2012;52:876-82.
- [Google Scholar]
- Physiotherapy for anterior knee pain: A randomised controlled trial. Ann Rheum Dis. 2000;59:700-4.
- [Google Scholar]
- Efficacy of home-based kinesthesia, balance and agility exercise training among persons with symptomatic knee osteoarthritis. J Sports Sci Med. 2012;11:751-8.
- [Google Scholar]
- Nondrug noninvasive treatment in the management of patellofemoral osteoarthritis. Indian J Med Sci. 2011;65:203-11.
- [Google Scholar]
- Effectiveness of retro walking in chronic osteoarthritis of knee joint. Innov J Med Health Sci. 2013;3:19-22.
- [Google Scholar]
- Supplementing a home exercise programme with a class-based exercise programme is more effective than home exercise alone in the treatment of knee osteoarthritis. Rheumatology (Oxford). 2004;43:880-6.
- [Google Scholar]




