
Translate this page into:
Validation of the Caregiving Knowledge Questionnaire-My: Measuring Knowledge Regarding Positioning and Feeding among Malaysian Informal Caregivers of Stroke Patients
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aim:
The majority of caregivers for stroke patients in Malaysia are informal caregivers, although there are no valid tools to measure their knowledge regarding caregiving. Therefore, this study validated the Caregiving Knowledge Questionnaire (CKQ-My) as an assessment of Malaysian stroke caregivers' knowledge regarding patient positioning and feeding.
Methods:
Back-to-back translation was used to produce a bilingual version of the questionnaire. Hand drawings were used to replace photographs from the original questionnaire. Face validity and content validity were assessed, and construct validity was determined by comparing responses from informal caregivers, medical students, and primary care doctors. Finally, the internal consistencies of the subscales were determined.
Results:
Pretesting showed that the translated version was sufficiently easy to understand. Internal consistency for the positioning subscale (28 items, Cronbach's α = 0.70) and feeding subscale (15 items, Cronbach's α = 0.70) was good. Mean scores for the positioning subscale for caregivers (mean: 17.1 ± 3.9), medical students (mean: 18.9 ± 3.1), and doctors (mean 21.5 ± 2.2) were significantly different (F = 5.28, P ' = 0.011). Mean scores for the feeding subscale for caregivers (mean 13.1 ± 2.5), medical students (mean 16.1 ± 1.9), and doctors (mean 16.1 ± 2.4) also differed significantly (F = 6.217, P = 0.006).
Conclusions:
CKQ-My has good internal consistency and construct validity for the subscales measuring stroke caregivers' knowledge about positioning and feeding of stroke patients. It has potential as an assessment of effectiveness of caregiver training and for future studies on long-term stroke outcomes in Malaysia.
Keywords
Caregivers
health knowledge
home nursing
stroke
validation studies

INTRODUCTION
Mostly family members take care of stroke patients in Malaysia.[12] These informal caregivers are more prone to negative effects on their health such as depression.[3] The burdens on caregivers can also affect the patients. To provide caregiving knowledge, transition care programs have been developed, which give structured caregiver training, postdischarge support, and follow-up. In Malaysia, most health facilities are yet to implement such training.[4] This study aimed to adapt and validate the Caregiving Knowledge Questionnaire (CKQ) among Malaysian informal caregivers.
METHODS
This was a validation study conducted at an urban teaching hospital in Malaysia. Permission was obtained from the original developer of the survey[5] to translate and adapt it for local use. The original survey was developed to measure knowledge of formal caregivers in Korea. It consisted of 31 items regarding knowledge about the positioning of patients, 6 items about feeding, 6 items about prevention of pressure ulcers, and 2 items about range of motion exercises.
The original survey items covered a range of tasks that most caregivers of dependent patients were expected to perform. Items for positioning scale comprised of pictures, making it easier for patients to select their responses. The questions were developed based on standard textbooks on rehabilitation and thus had some degrees of content validity. However, the initial questions did not have a uniform scoring method and some questions had more than one potential answer. Findings from the original version were, therefore, presented as percentages of correct answers. Hence, the tool required some modification and psychometric validation to be justifiably used as a scale to measure caregiving knowledge.
The validation study was conducted in two phases. The first phase involved translation and adaptation of the questionnaire to suit the local setting. The second phase involved determining the internal consistency and the ability of the measure to distinguish between contrasting groups.
Ethical consideration and informed consent
All participants received a briefing as to the purpose of the study and written informed consent was obtained. All identifying data were replaced with participant numbers during analysis. The study received ethical approval from the Institutional Medical Research and Ethics Committee (FF-2017–196).
Translation and adaptation of the questionnaire
The original survey items were reviewed by the research team for grammatical errors. The initial content review also led to the two items for range of motion exercises to be removed from the questionnaire. This was because upon discussion with a trained physiotherapist and search for guidelines, the questions were deemed invalid since there is no evidence-based recommendation about the ideal frequency of range of motion exercises for stroke patients.[6] The locations of range of motion exercises would also depend on the location of the disability, and hence it would be inappropriate to assess the knowledge of caregivers on locations of range of motion exercises if the patient they cared for did not have disability at certain joints.
Hand drawings replaced the original photographs to ensure that the pictures could be easily reproduced in black and white and also to relabel the affected limbs. This also minimizes ethical issues related to photographs and would be more acceptable in a Muslim-predominant country. Hand drawings are also easier and cheaper to reproduce compared to photographs. The corrected version was then sent to be translated by two independent translators to obtain the Malay version. The Malay version was reviewed by the research team members and reconciled to produce a harmonized version. The research team members were all competent users of Malay and English language; five of the team members were native speakers of Malay. Differences in the terms were reconciled through discussions and final consensus. This harmonized version was subsequently sent to another two independent translators who translated it back into English. Finally, all language versions were compared by the research team members with the original version to ensure semantic and conceptual equivalence.
The harmonized Malay version was then pretested among five caregivers of stroke patients. Pretesting usually requires between 5 and 15 samples and are best done in a heterogeneous population.[7] Further modifications were made, based on pretesting results, to improve the flow of the language and explanatory phrases were added where necessary. Some local cultural examples were given. For example, an answer option to the item on the correct consistency of milk “like yogurt drink” was elaborated by giving examples of popular local brands of yogurt drinks. The amended version was pretested on another two participants and was approved for the validation phase.
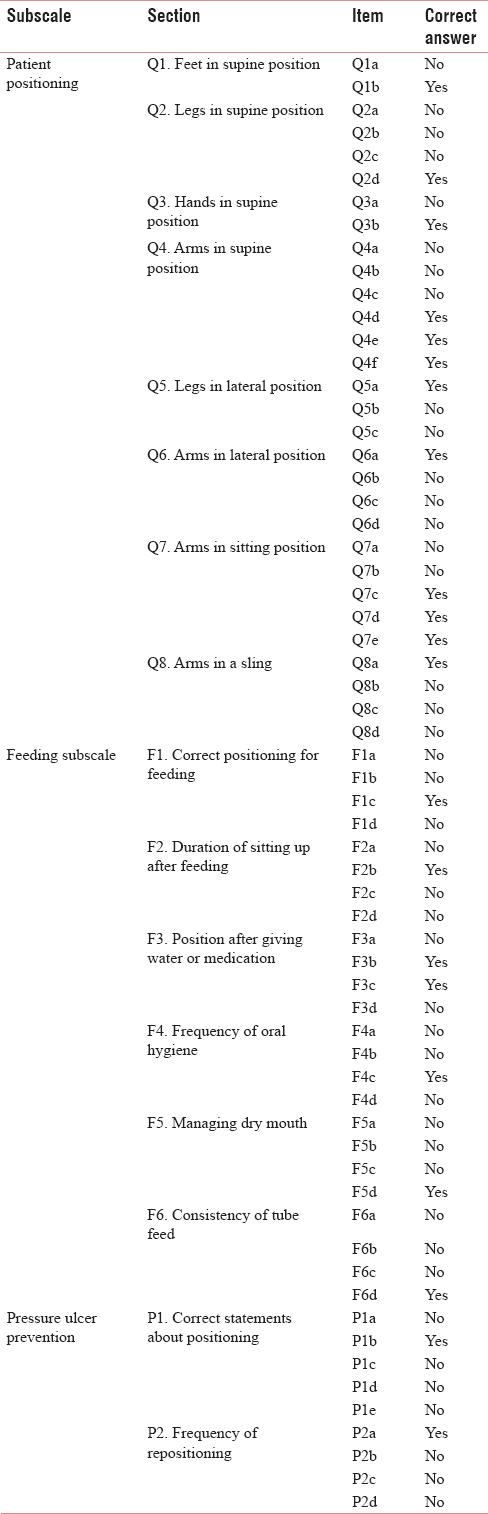
There were a total of thirty items in the patient positioning subscale, 25 items in the feeding subscale, and 9 items in the pressure sore prevention subscale. Separate sections could have more than one correct response. Hence, each correct answer was awarded 1 point. Respondents were also awarded marks for not selecting incorrect items. No marks were deducted for wrong answers. Respondents who were not involved in feeding the patient through a tube were exempted from answering the feeding subscale but were required to complete all other sections. Table 1 shows the breakdown of items in the questionnaire used for validation.
Validation procedure
In view that there were no prior gold standard questionnaires to allow concurrent validation, we used contrasting groups validation method. In contrasting groups' validation, the samples for each group are purposively recruited to form a priori groups.[8]
The developed questionnaire was tested on 13 caregivers of stroke patients (ages 30–74 years, 9 females and 4 males) using convenience sampling from a long-term stroke clinic. The questionnaire was also self-administered to 10 4th year medical students (8 females and 2 males, aged between 24 and 26 years) and ten primary care doctors (8 females and 2 males, aged between 30 and 38 years, and who were in their 2nd and 3rd years of training in family medicine).
Internal consistency and contrasting groups' discrimination analyses
The internal consistency was determined for each predetermined subscale, namely, patient positioning, feeding, and pressure sore prevention. Items with no variance or had poor item-total correlations were removed. Items that improved the internal consistency when deleted were also removed one by one until a satisfactory internal consistency was achieved. The subscale for pressure sore prevention, however, failed to achieve a satisfactory internal consistency due to the presence of too few items, and thus the subscale was removed from the questionnaire.[9]
The total scores for the subscales were calculated based on the final 29 items for the patient positioning subscale and 15 items for the feeding subscale. The contrasting group method was used to determine the questionnaire's construct validity. Theoretically, informal caregivers should have lower knowledge compared to medical students and doctors. Hence, a significant difference in scores between these three groups would support the tool's ability to discriminate between good and poor knowledge in this domain.
RESULTS
Only two caregivers did not complete the feeding subscale of the CKQ-My. Table 1 shows the correct answers for each item in the patient positioning subscale and the feeding subscale.
Patient positioning subscale
The initial Cronbach's alpha for this subscale was 0.637 [Table 2]. From the initial 30 items, items Q2a and Q4b were dropped. Item Q2a referred to the placement of a pillow under the patient's knees while lying supine, whereas Q4b referred to use of an arm sling while lying supine. Theoretically, removing items from each question may affect the difficulty level of the questions as the number of possible options is reduced. It is also important to retain correct positioning options. Dropping items Q2a and Q2b did not remove the correct answers and kept at least two items to be considered by the participants.

Feeding subscale
The initial Cronbach's alpha was 0.544 for the preliminary 24 items. Items with poor item-total correlation were removed one by one to improve the internal consistency. The final Cronbach's alpha for the feeding subscale was 0.695 after dropping five items. Again, before removing the items, care was taken to ensure that items representing correct feeding knowledge were not inadvertently removed from the questions. Each question also had at least three options to choose from to preserve its difficulty index.
Pressure ulcer prevention subscale
Cronbach's alpha for the pressure ulcer prevention subscale was extremely low (0.327). This may have been due to an insufficient number of items in the subscale.[9] To improve the subscale, it is thought that more items related to pressure ulcer prevention would need to be developed and tested. Hence, the subscale for pressure ulcer prevention was removed from the questionnaire in the current study.
Contrasting groups validity
The scores for each subscale were summed. The overall mean score for the patient positioning subscale was 20.30 ± 3.72, whereas overall mean score for the feeding subscale was 10.57 ± 2.30. The scores of both subscales were normally distributed and are displayed in Table 3. Overall, there was a significant difference in mean scores between the different groups.

Post hoc tests [Table 4] revealed significant mean differences between caregivers' scores and doctors' scores for both the patient positioning and feeding subscales. Caregivers' scores for feeding were also significantly lower than medical students' scores. Medical students' and doctors' mean scores for feeding were comparable.

DISCUSSION
The CKQ-My had satisfactory internal consistency (that is, a Cronbach's alpha of at least 0.70) and contrasting groups' validity in measuring caregiving knowledge among Malaysian caregivers for stroke patients.[9] It has the potential to be used for assessing effectiveness of caregiving training in two areas of basic caregiving, which are positioning of the patient and feeding. To date, this is the first validated tool to measure caregiving knowledge in Malaysia.
The patient positioning subscale is pictorial in nature, making it easy to administer. Pictures of various positions aid respondents to complete the section, as opposed compared to sentences. Respondents are allowed to choose as many correct answers as they like. Therefore, they are also awarded scores for not choosing incorrect items. This prevents scores from being awarded for guessing, as the probability of choosing a correct answer is 50% for each item.
Items in the feeding subscale are comprised of simple sentences about basic steps in feeding the patient. Another tool, the Home Enteral Nutrition Caregiver Task checklist, is much more detailed.[10] The Home Enteral Nutrition Caregiver Task, however, does not measure only knowledge but includes the assessment of caregivers' practices in providing enteral nutrition to the patient, encompassing how they manage complications, and other associated tasks. Adding additional items to the current My-CKQ such as the management of possible complications may test a higher level of knowledge. Future modifications and psychometric testing could also further improve the feeding subscale.
Unfortunately, the pressure ulcer prevention subscale did not have adequate internal consistency and was, therefore, removed. This is most likely to be due to the inadequacy of items within the subscale.[9] Prevention of pressure ulcers involves addressing various factors such as the patient's positioning, nutritional status, skin care, transfer techniques, as well as frequency of repositioning.[11] Caregivers' knowledge on all these aspects should be assessed to form a valid and reliable assessment tool. Most studies regarding pressure ulcers and prevention have been conducted among health-care professionals.[1213] However, the knowledge of caregivers has not been studied. This is an important component of caregiver knowledge which needs to be addressed, as most informal caregivers do not receive adequate training regarding prevention of pressure ulcers, resulting in higher caregiving burden.[1415]
To the best of our knowledge, this is the first validation study of a tool designed to assess knowledge of informal caregivers regarding care for a stroke patient. The original survey by Lee et al. was designed to assess the knowledge of trained caregivers. However, with some modifications, the tool was tested on informal caregivers and found to be easily understood and applicable to the local Malaysian population. The pictorial form of items for the patient positioning subscale facilitates respondents in completing the section. Both subscales were deemed to have adequate internal consistency and discriminative validity.
The CKQ-My, however, has some limitations. It only assesses caregivers' knowledge on positioning and feeding. Hence, more items need to be developed to assess knowledge on other aspects of caregiving such as pressure ulcer prevention. The feeding subscale may also be further improved by adding items on important precautions to avoid complications and how to manage complications. Further testing in the Malaysian population will also provide data for population norms and add to the establishment of the validity of this tool.
CONCLUSIONS
The CKQ-My is a valid and reliable tool to measure the knowledge of Malaysian informal caregivers of stroke patients, in aspects of patient positioning and tube feeding. The tool has also potential to be used for assessing the effectiveness of caregiver education programs.
Financial support and sponsorship
Partial funding was received from the Universiti Kebangsaan Malaysia (Grant No: GGP-2017-019). No further funding from the public, commercial, or not for profit sectors was received.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to acknowledge UKMMC Long-Term Stroke Clinic, and the Department of Medical Rehabilitation Services for their roles in supporting the validation process. We would also like to thank the staff of the Long-Term Stroke Clinic for support rendered and Editage team for English language editing. The authors also thank the Director-General of Health, Malaysia, for permission to publish this paper.
REFERENCES
- The formal and informal long-term caregiving for the elderly: The Malaysian experience. Asian Soc Sci. 2013;9:174-84.
- [Google Scholar]
- Projecting social support needs of informal caregivers in Malaysia. Health Soc Care Community. 2014;22:144-54.
- [Google Scholar]
- Family caregiving for patients with stroke. Review and analysis. Stroke. 1999;30:1478-85.
- [Google Scholar]
- Care for post-stroke patients at Malaysian public health centres: Self-reported practices of family medicine specialists. BMC Fam Pract. 2014;15:40.
- [Google Scholar]
- A survey of caregivers' knowledge about caring for stroke patients. Ann Rehabil Med. 2015;39:800-15.
- [Google Scholar]
- Treatment interventions for the paretic upper limb of stroke survivors: A critical review. Neurorehabil Neural Repair. 2003;17:220-6.
- [Google Scholar]
- Cognitive interviewing for item development: Validity evidence based on content and response processes. Meas Eval Couns Dev. 2017;50:217-23.
- [Google Scholar]
- Procedures for assessing the validities of tests using the “known-groups” method. Appl Psychol Meas. 1984;8:295-305.
- [Google Scholar]
- Family caregivers of older adults on home enteral nutrition have multiple unmet task-related training needs and low overall preparedness for caregiving. J Am Diet Assoc. 2004;104:43-50.
- [Google Scholar]
- Preventing pressure ulcers: The goal is zero. Jt Comm J Qual Patient Saf. 2007;33:605-10.
- [Google Scholar]
- A survey of australian nurses' knowledge of pressure injury/Pressure ulcer management. J Wound Ostomy Continence Nurs. 2015;42:450-60.
- [Google Scholar]
- Educational campaign to increase knowledge of pressure ulcers. Br J Nurs. 2016;25:S30-5.
- [Google Scholar]
- Keeping vulnerable elderly patients free from pressure ulcer is associated with high caregiver burden in informal caregivers. J Eval Clin Pract. 2010;16:585-9.
- [Google Scholar]
- Informal carers and wound management: An integrative literature review. J Wound Care. 2015;24:489.
- [Google Scholar]




