
Translate this page into:
Professional Quality of Life among Professional Care Providers at Cancer Palliative Care Centers in Bengaluru, India
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Being a professional care provider at cancer palliative care settings is demanding and stressful. Literature has indicated the prevalence of high burnout (BO) and distress; however, there is a dearth of studies in India, with no study available on professional quality of life in the field of palliative care.
Aims:
The aim of the present study was to explore the professional quality of life, namely-compassion satisfaction [CS], burnout [BO], and secondary traumatic stress [STS] among professional care providers at cancer palliative care centers.
Settings and Design:
A cross-sectional, descriptive, and quantitative study was carried out at four cancer palliative care centers in Bengaluru after the permissions and ethical approvals.
Subjects and Methods:
The tools used were brief sociodemographic datasheet and professional quality of life (ProQoL)-Version 5 administered with 65 participants (mean age = 32.5 and standard deviation = 11.78) with work experience of at least 6 months.
Analysis:
A descriptive, correlational, and inferential analysis of the quantitative data was undertaken.
Results:
The results revealed that an average level of CS and BO was reported by 32 (49.2%) and 35 (53.8%) study participants, respectively, while 62 (95.4%) participants reported higher STS on ProQoL scale-Version 5. Significant differences in levels of CS, BO, and STS were found based on additional training taken in palliative care (P = 0.01), designation type (P < 0.001), and workplace type (P = 0.01).
Conclusion:
The overall results strongly suggest that a short intervention targeting STS and BO can help the study population and further enhance their CS and patient care.
Keywords
Burnout
compassion satisfaction
palliative care professionals
secondary traumatic stress

INTRODUCTION
The very essential unit of the palliative care is the “professional care provider” working in a multidisciplinary setup to provide holistic care in the physical, psychological, spiritual, and environmental domains of the patient as well as their family members. With the aim of “death with dignity” and the holistic care, palliative care is provided by a team of physicians, nurses, and other health professionals who work together with the primary care physician and referred specialists (or, for patients who do not have those, hospital or hospice staff) to provide an extra layer of support.[1] About one-third of those needing palliative care suffer from cancer.[2]
India's large growing population and a noteworthy rise of advanced-stage illness diagnoses such as cancer are presenting significant demands on palliative care;[3] moreover, most cancer patients seek treatment during the advanced stages in India.[4] The professional skills required for caring for the dying are different from caring for other patients.[5] Working as a professional care provider with patients who have advanced cancer has many rewards, but can also be challenging and stressful.[67] The compassionate care provided by these professionals makes them different when the patient has been told “nothing can be done now” by professionals at other settings.[8] However, the same compassionate care can serve as a major source of psychological stress in their lives. This makes them vulnerable to experiencing burnout (BO) and/or compassion fatigue, both at an individual and at a team level.[910]
Although symptoms of BO and compassion fatigue are similar,[11] BO stems from work-related stressors while compassion fatigue is a relational source of stress.[12] There is limited research on compassion satisfaction (CS), secondary traumatic stress (STS), and areas of work life. Most of the literature till date has focused on areas of work life and BO.[13] Research suggests that cancer palliative care professionals are at risk for developing negative consequences for themselves as well as the patient care.[69] Despite the need to address these challenges, there is a dearth of studies in the field of palliative care in India, with only few exploratory studies published [381415] and not even a single study on professional quality of life domains, namely, CS, BO, and STS in cancer palliative care professionals.
The aim of the present study was to study the professional quality of life among professional care providers at cancer palliative care centers. The study objectives were (a) to study the prevalence of CS, BO, and STS in professional care providers at cancer palliative care centers and (b) to study the associations of demographic and work-related characteristics with CS, BO, and STS in professional care providers at cancer palliative care centers.
SUBJECTS AND METHODS
Sample
The study was cross-sectional, quantitative, and descriptive in nature. The target population for the current study was professional care providers working full-time and providing direct care to patients at different cancer palliative care centers in Bengaluru. Sample size estimation was calculated for the current study using estimates from a previous study.[12] For a margin of error of 2 units and level of significance of 5%, the estimated minimum sample size was found to be 50. Inclusion criteria of the participation were as follows: (1) professionals (doctor, nurse, counselor, psychologist, social worker, pharmacist, or physiotherapist) working at any cancer palliative care center in Bengaluru; (2) professionals involved in direct patient care at cancer palliative care center; (3) professionals with work experience in palliative care for at least 6 months; and (4) professionals who have the ability to read and write in English or Hindi.
Procedure
The study commenced after the approval from the Protocol Review Committee (Behavioural Sciences) and Institute Ethics Committee (IEC), National Institute of Mental Health and Neurosciences, Bengaluru, Karnataka, India. Furthermore, permissions and ethical approval was obtained from the four cancer palliative care centers (one hospice and three hospitals) before initiating the study. The sample for the present study was recruited using purposive sampling method. A total of 98 professionals were available at the time of the study at the four centers; however, 31 did not meet the criteria for the study (language, work experience, and indirect care). A total of 67 participants who met inclusion criteria were called and personally contacted (phone calls and e-mails) from the four cancer palliative care centers in Bengaluru with the help of coordinators at each center. Of the 67 participants contacted, 65 participants gave written informed consent for participation in the study.
Tools
The tools used were as follows: (1) brief sociodemographic datasheet which was developed for the study by the researcher to collect information about sociodemographic details, professional details, and nature of work information and (2) professional quality of life (ProQoL)-Version 5 Stamm, which is used to collect data on BO, STS, and CS. ProQoL R-5 is a recent simpler instrument comprised of 30 questions, which includes a 6-point Likert scale (0 = never and 5 = very often).[16] Three subscale scores included BO, STS, and CS. The instrument has been tested with reliability α (CS = 0.87, BO = 0.72, and compassion fatigue = 0.80). Each subscale is unique, and the results of the scales cannot be combined to give a single meaningful score. Construct validity has been well established by Stamm. The tools and written informed consent were translated and back-translated into Hindi.
Data analysis
Data analysis was carried out using IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. Frequency distributions of all the variables were checked for outliers, missing data, and typing errors. Summary statistics, including the computation of means, standard deviations (SDs), frequency counts, and percentages of all demographic and professional data, were performed. Means, SDs, and percentages were computed for the level of CS, BO, and STS. Shapiro–Wilk test for normality was carried out to note the normality of the distribution. One-way analysis of variance (ANOVA) was used to compare the mean scores on CS, BO, and STS on the basis of designation type, while independent sample t-test was used to compare the mean scores on the basis of workplace type, gender, and additional training taken in palliative care. Pearson's r correlation was calculated to study the significant relationship between CS, BO, and STS with age, number of cases seen per week, income per month, and number of years spent as work experience in palliative care. P ≤ 0.05 was considered statistically significant.
RESULTS
Demographic, professional, and work-related characteristics
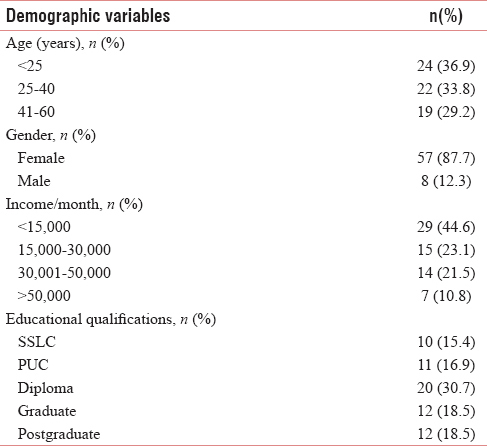
The mean age of the study population was 32.5 years (SD = 11.78), ranging from 18 to 60 years of age. The participants of the study were primarily women (n = 57, 87.7%), with the majority falling under 25 years of age (n = 24, 36.9%), and 29 professionals (44.6%) earning ≤15,000 rupees/month. Twenty participants of the study population (n = 65) had completed a diploma (nursing/pharmacy/counseling), while 12 participants (18.7%) were educated till graduation and postgraduation each [Table 1].
Years of working as a professional care provider in palliative care ranged from 6 months to 21 years (M = 3.8; SD = 3.88). Cases seen per week (M = 27.5; SD = 18.04) ranged from 5 cases to 87 depending on the designation and workplace type. Mean number of hours worked daily at workplace was 8.1 h (SD = 0.83). The different professional care providers in the current study consisted of 21 nurses (32.3%), 18 nursing aids (27.7%), 14 doctors (21.5%), 6 counselors (9.2%), 3 social workers (4.6%), and 3 others (4.6%; 1 pastor, 1 physiotherapist and 1 pharmacist). These professionals were grouped in three after matching their characteristics.
Workplace type in palliative care included 43 professionals working at a hospice (66.2%) and 22 working at hospitals (33.8%). Of the 65 participants, only 34 (52.3%) professionals had taken an additional training in palliative care in the form of degree, diploma, certificate course, fellowship, workshops, and observership, while 31 (47.7%) had no training in any form in the area of palliative care [Table 2].

Magnitude of compassion satisfaction, burnout, and secondary
The raw scores obtained on CS, BO, and STS were converted into T-scores as per Stamm's (2010) interpretation. The mean scores of the study population for the level of CS, BO, and STS among professional care providers at cancer palliative care centers were 54.6 (SD = 6.55), 54.9 (SD = 6.01), and 70 (SD = 6.97), respectively. Thirty-two professionals (49.2%) fell into the average level of CS (between 25th and 75th percentile), and 35 professionals (53.8%) scored within the average level of BO, while 62 professionals (95.4%) scored above 75th percentile on STS [Table 3].

Associations of demographic and work-related characteristics with compassion satisfaction, burnout, and secondary traumatic stress
Significant negative correlation was found between CS and BO (P< 0.01), while a positive correlation was significant between BO and STS (P< 0.01). In a correlation between CS, BO, and STS with age and income per month (demographic), no significant relationship was seen. However, with work-related characteristics such as number of years spent in palliative care and cases seen per week, significant correlations were seen. CS was found to have a significant positive correlation with the number of years in palliative care (P< 0.05) while the number of cases seen per week was found to have a negative correlation with BO (P< 0.05) and a positive correlation with STS (P< 0.05) [Table 4].

For a better understanding of the associations between CS, BO, and STS with other important study participants' characteristics (designation type, workplace type, gender, and additional training taken), t-test and one-way ANOVA were carried out after Shapiro–Wilk normality test. It was seen that nurses and nursing aids had significantly higher BO (F = 3.34, P = 0.04) and STS (F = 9.92, P < 0.001) than the other professionals. Professionals working at hospice were seen to have significantly higher STS (t = 2.53, P = 0.01) than professionals working at hospital settings. There were no significant differences found on scores on CS, BO, and STS based on gender. Professionals who had reported having undergone additional training in palliative care had significantly higher CS (t = 2.58, P = 0.01) than those who had no training.
DISCUSSION
Professional quality of life has grown as an interesting topic of interest in the recent past with the development of better validated scales in the context of helping professionals. Several studies have been published previously on the prevalence of BO in the western literature, while compassion fatigue is relatively new. The “cost of caring” or compassion fatigue seems to be an important area to be highlighted through more studies as the psychological and physical health of professionals can have potential consequences on the quality of care provided to the patients.
The field of palliative care in India is still growing, and with limited health-care resources, scarcity of trained professionals, and rise in advanced stage cancer patients, the demands are increasing with the burden on the palliative care professionals.[3417] In such a scenario, providing support to the professionals working in the field of palliative care becomes utmost important and need of the hour. However, in India, the current study is the first attempt to study professional quality-of-life domains, namely CS, BO, and STS in professional care providers at cancer palliative care centers.
In this study, results indicated an average level of CS and BO while very high STS. Almost half of the study population reported having an average level of CS, while nearly half of the study population reported having higher CS (scores above 75th percentile), which indicates that more than half of the total study population was able to derive optimum pleasure from their work. The study findings may also indicate that participants felt positively about helping others which could be culture-related beliefs about altruism as they might feel they are doing greater good for the society. Similarly, little more than half of the study population reported having an average level of BO, while nearly half of the study population reported having higher BO (scores above 75th percentile), which indicates that they might be “at risk” as individuals. This could be the result of many personal and organizational factors which are usually work related. The workload (cases seen per week) varied within the sample and BO effects generally include exhaustion, feelings of unhappiness, bogged down, and being overwhelmed. Only six professionals had lower levels of BO from the study population which is very less in number.
STS, which was earlier known as compassion fatigue or vicarious traumatization, makes individuals fearful and helpless. According to Stamm, a combination of high STS and high CS and moderate-to-low BO indicates that such professionals are highly effective at their work because they feel their work matters; however, engagement with other's trauma leads to a private fearful self.[16] High STS can be seen very evidently in the present study population, with 62 professionals falling above the 75th percentile and it indicates that they may need some immediate intervention [16] for their secondary exposure to extreme or traumatically stressful events. Furthermore, the prevalence of BO and STS would most likely continue to rise till some solutions are made available to decrease its severity.[18] The results for BO were similar to the findings from some previous studies [819] where cancer palliative care professionals had high stress, high BO, and poor quality of life. It was found that results obtained for CS and STS were consistent with a recent study done with professionals from Brazil and Spain by Galiana et al. (2017); however, BO findings are inconsistent in comparison to this study.[20] The current study finding of high STS with majority of study population scoring above the 75th percentile is serious and different from findings from other studies [21] where only some professionals crossed the top quartile range on STS. In the current study, of 62 professionals scoring in the top quartile (75th percentile), 12 had scored above the cutoff which raises an alarm for some immediate help.
In the present study, a stronger and statically significant negative correlation was found between CS and BO rather than CS and STS which is consistent with findings from other studies.[2223] A low BO would indicate low STS and high CS based on correlation results in the current study. The positive significant correlation between BO and STS might also lead to suboptimal patient care.[24]
In a correlation between CS, BO, and STS with age and income per month (demographic), no significant relationship was found which is consistent with earlier studies where no relationship was found between CS, BO, and STS with age.[25] These findings are different from other studies [1323] where they observed BO had some relationship (positive or negative) with age of the palliative care specialists. The current findings might be because of heterogeneous sample as majority reported having moderate-to-high CS and most from the study population also have <15,000 international normalized ratio income per month. However, CS was found to have a significant positive correlation with the number of years of work experience in palliative care, which indicates more experienced the professional is in the field, more pleasure he/she will derive from doing the job well. The number of cases seen per week was found to have a negative correlation with BO and a positive correlation with STS, which is quite interesting as it indicates that professionals who ended up taking care of more number of cases per week had low levels of BO and high levels of STS in the present study. The latter finding could be understood in terms of more the workload more would be the aftereffects of the same. Furthermore, it was observed that experienced professionals had more number of cases as compared to the young and comparatively less experienced professionals, which could also mean that former group's satisfaction is high and BO is low.
Levels of CS, BO, and STS were compared on the basis of designation type, workplace type, gender, and additional training taken in the present study. Results indicated that nurses and nursing aids had significantly higher BO and higher STS than the other professionals, which is consistently seen in other studies. Previous researches have indicated that nurses experience more physical symptoms, low accomplishment,[26] more BO, and high work stress,[27] and risk of compassion fatigue is higher in nurses.[102829] The possible explanations for experiencing more psychological distress could be because nurses are supposed to spend more time with the patients as compared to other professionals; they tend to encounter more deaths and high-risk situations at workplace.
Professionals working at hospice were seen to have significantly higher STS than professionals working at hospital settings, which is consistent with the findings from earlier studies.[29] Earlier studies have reported that women professionals reportedly are more likely to exhibit STS, have lower sense of accomplishment and experience greater distress in palliative care,[2630] while in the present study, no significant differences were found on the scores on CS, BO, and STS based on gender. Professionals who had reported having undergone additional training in palliative care had significantly higher CS which is supported by a previous study [30] which stated specialized training increased levels of CS. Furthermore, another possible explanation for trained professionals having higher satisfaction could be the knowledge of alternatives and confidence of handling difficult situations. Being a professional in palliative care is said to be challenging and needs different skills than other setups, and the present study data raise the need for more training opportunities. Better training and supervision facilities could mean better care for the patients and their families.
While this is the first known study on professional quality of life among professional care providers at cancer palliative care centers in Bengaluru, it is limited by its sample size of 65 participants. In addition, the prevalence of CS, BO, and STS were measured cross-sectionally, and there is a possibility that an individual's assessment of his/her perceptions can change over time due to individual work-related conditions.[16] Moreover, the PRoQoL scale is a self-report scale where ratings for each statement are subjective and perceptions of various work-related variables in the present population could be studied further.
The findings from the present study can have a positive impact on the future research in the field. This is the first step toward addressing the needs and challenges experienced by the professionals with respect to their work life, and similar studies could be carried out in other regions within India to explore the construct more. The professionals working in cancer palliative care settings could benefit from a psychosocial capacity-building intervention that reduces the risk for compassion fatigue, enhance their well-being, and equip them with better strategies to handle difficult life and death situations at workplace. This will further benefit the cancer palliative care centers as quality of patient care would improve as an end-result with no additional costs involved. This study also highlights the need for more training opportunities and psychological care for the professionals to be included within the training modules or programs.
CONCLUSION
The findings from the present study strongly suggest that professional care providers working at cancer palliative care centers need a brief intervention program which could target decreasing their BO and STS levels and further enhance their CS.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Senior Officials from Karunashraya, Bangalore Hospice Trust; Palliative Care Department Heads from St. John's Medical College and Hospital, Kidwai Memorial Institute of Oncology and Bangalore Baptist Hospital. Special thanks to Ms. Maria Sonia and Dr. Jeremy Johnson from Karunashraya.
REFERENCES
- History of psycho-oncology: Overcoming attitudinal and conceptual barriers. Psychosom Med. 2002;64:206-21.
- [Google Scholar]
- First Ever Global Atlas Identifies Unmet Need for Palliative Care. Available from: http://www.who.int/mediacentre/news/releases/2014/palliative-care-20140128/en/
- Views on death and dying among health care workers in an Indian cancer care hospice: Balancing individual and collective perspectives. Palliat Med. 2012;26:250-6.
- [Google Scholar]
- The organizational context of dying. In: Death the Final Stage of Growth. Englewood Cliffs, NJ: Prentice Hall; 1975. p. :7-26.
- [Google Scholar]
- EPEC-O: Education in palliative and end-of-life care for oncology. Module. 2005;2:12-4.
- [Google Scholar]
- The transformation process for palliative care professionals: The metamorphosis, a qualitative research study. Palliat Med. 2016;30:161-70.
- [Google Scholar]
- Stress, Coping and Quality of Life among Staff Working in Palliative Care.(Unpublished Master's Thesis). Bangalore, India: National Institute of Mental Health and Neurosciences; 2005.
- Self-care of physicians caring for patients at the end of life: “Being connected… A key to my survival”. JAMA. 2009;301:1155-64.:E1-64.
- [Google Scholar]
- Adverse psychosocial consequences: Compassion fatigue, burnout and vicarious traumatization: Are nurses who provide palliative and hematological cancer care vulnerable? Indian J Palliat Care. 2008;14:23.
- [Google Scholar]
- Compassion fatigue: Psychotherapists' chronic lack of self care. J Clin Psychol. 2002;58:1433-41.
- [Google Scholar]
- Compassion fatigue and burnout: Prevalence among oncology nurses. Clin J Oncol Nurs. 2010;14:E56-62.
- [Google Scholar]
- Compassion satisfaction, compassion fatigue, work life conditions, and burnout among frontline mental health care professionals. Traumatology. 2013;19:255-67.
- [Google Scholar]
- Nurses attitudes toward palliative care for cancer patients. Nurs Midwifery Res. 2005;1:47.
- [Google Scholar]
- A critical ethnography of oncology palliative care nurses in India: Exploring the relationship between moral distress and cancer pain management (S765) J Pain Symptom Manage. 2014;47:505-6.
- [Google Scholar]
- 2010. The Concise Manual for the Professional Quality of Life Scale. Pocatello, ID: ProQOL.org. Available from: https://www.proqol.org/.
- Development of palliative care in India: An overview. Int J Nurs Pract. 2006;12:241-6.
- [Google Scholar]
- Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. J Nurs Scholarsh. 2015;47:186-94.
- [Google Scholar]
- Burnout syndrome in the practice of oncology: Results of a random survey of 1,000 oncologists. J Clin Oncol. 1991;9:1916-20.
- [Google Scholar]
- Compassion satisfaction, compassion fatigue, and burnout in Spain and Brazil: ProQOL validation and cross-cultural diagnosis. J Pain Symptom Manage. 2017;53:598-604.
- [Google Scholar]
- Compassion satisfaction, compassion fatigue, anxiety, depression and stress in registered nurses in Australia: Study 1 results. J Nurs Manag. 2014;22:506-18.
- [Google Scholar]
- Secondary traumatic stress and oncology social work: Protecting compassion from fatigue and compromising the worker's worldview. J Psychosoc Oncol. 2005;23:1-4.
- [Google Scholar]
- Burnout and psychiatric disorder among cancer clinicians. Br J Cancer. 1995;71:1263-9.
- [Google Scholar]
- Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136:358-67.
- [Google Scholar]
- Secondary traumatic stress, burnout, compassion fatigue and compassion satisfaction in trauma nurses. Am J Crit Care. 2009;18:e1-7.
- [Google Scholar]
- Work-related stress specific to physicians and nurses working with cancer patients. J Psychosoc Oncol. 1992;10:79-99.
- [Google Scholar]
- Predicting the risk of compassion fatigue: A study of hospice nurses. J Hosp Palliat Nurs. 2006;8:346-56.
- [Google Scholar]
- Compassion fatigue, compassion satisfaction, and burnout: Factors impacting a professional's quality of life. J Loss Trauma. 2007;12:259-80.
- [Google Scholar]




